
Tag: Nursing Assessment
Articles about the nursing assessment often dealing with a terminally ill patient and the goals of maintaining comfort at the end-of-life.
Articles about the nursing assessment often dealing with a terminally ill patient and the goals of maintaining comfort at the end-of-life.
I know how important it is to provide comfort and support during this challenging journey. One aspect of hospice care that often raises concerns is deprescribing medications. In this article, we'll explore what deprescribing is and why it can benefit patients nearing the end of life.
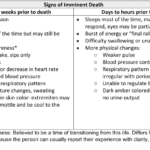
Recognizing end-of-life signs can be challenging. This guide outlines key symptoms indicating a terminally ill patient may have less than two weeks, offering crucial insights for caregivers and families.

Losing a loved one is an incredibly challenging experience, and witnessing changes in their behavior and well-being can be distressing. As a hospice nurse, I've supported many families and caregivers through this grim time. One common symptom that may arise towards the end of life is restlessness. In this article, I will explain the different types of restlessness and offer guidance on how to manage them. Understanding these distinctions can provide valuable insights into your loved one's condition and help you navigate the final stages of their life with compassion and care.

Heart failure is a complex medical condition that can impact the quality of life of patients, especially those in hospice care. As a hospice nurse, assessing the heart failure stage is crucial to providing appropriate care accurately. This article will explore the New York Heart Failure Classification System, its stages, and how to assess patients for their stages. Additionally, we will emphasize the importance of documentation in compliance with Medicare guidelines for terminally ill patients with heart failure.
Explore the journey of functional decline in the natural dying process. This article provides insight for caregivers and families, emphasizing the importance of documenting changes to enhance care and decision-making in life’s final chapter.

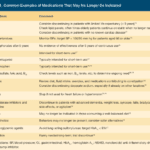
Medication reconciliation plays a pivotal role in hospice care, ensuring terminally ill patients receive safe medication regimens. This process involves maintaining an accurate medication list to prevent adverse drug events. It's essential at various stages, including admission, recertification, and changes in condition. Healthcare professionals should be familiar with tools like the Beers Criteria and STOPP/START criteria to identify potentially inappropriate medications and prescribing omissions in older adults.

Serotonin syndrome is a potentially life-threatening condition caused by an excess of serotonin in the body. Detecting this condition early is crucial, but it can be particularly challenging when dealing with dementia patients due to communication barriers and the complexity of their symptoms. In this article, we will present three case studies that highlight the early detection and successful management of serotonin syndrome in patients with different types of dementia: Alzheimer's disease, vascular dementia, and Lewy Body Dementia.

Hospice nurses assess the status of the patient's journey towards the end of life every nursing visit. Situations where a reversible condition can drastically impact the patient and the hospice assessment can occur. If it is not caught, it is potentially mistreated, leading to increased discomfort and a faster death, often involving increased suffering. One of the common clues that someone is getting closer to dying is increased agitation and restlessness.
Are you aware of Serotonin Syndrome?

Dementia is a condition that affects millions of people worldwide, and it can cause a range of symptoms, including pain and discomfort. Unfortunately, pain is often under-detected and undertreated in people with dementia, leading to significant suffering and a reduced quality of life. In this article, we will explore the prevalence of pain among dementia patients, the impact of unmanaged pain on their quality of life, behavioral changes that may indicate pain, and the use of the PAINAD pain scale as a tool for assessing and managing pain in dementia patients.
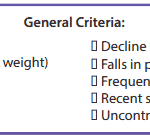
It’s essential to familiarize yourself with the key local coverage determination (LCD) facts for different terminal illnesses to avoid admitting patients who are not eligible for services only to be required to refund the money back to Medicare; otherwise, only have the patient on for one benefit period then discharged for failure to decline. These determinations provide guidelines on the coverage of hospice services for specific conditions. If you are the admitting nurse, please do not just admit because you were told to admit by someone, regardless of the position or standing of the person or party that told you to admit. Use your critical thinking and clinical judgment skills to evaluate the patient for admission. Most doctors will write "evaluate and treat" or something to that effect; never lose sight of the "evaluate" portion of the doctor's order.
Based on the provided PDF files, as noted in the resources section below, let’s explore some essential information for each terminal illness.
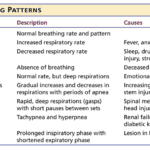
Understanding the final breath: This article explores the critical breathing patterns observed in the last hours of life, offering insights for caregivers and family members to prepare for the end-of-life journey.

One of the hardest portions of the job of a hospice nurse is to identify when a patient has two weeks of life left to live; this can be especially difficult at facilities going through staffing shortages leading to inconsistent caregivers with little to verbally report on a patient’s change of condition. Since being aware of the velocity of declines is extremely important, let’s cover an area that we in hospice (nurses, families, and caregivers alike) can keep an eye on in terms of identifying terminal restlessness which is often a key indicator for one week or less of life.

One of the most important roles is detecting and managing infections in terminally ill geriatric patients with dementia. These patients are often at higher risk for infections due to their weakened immune systems, underlying health conditions, and limited mobility. Detecting infections in these patients can be challenging due to their limited communication abilities and other cognitive and physical impairments. However, early detection and management of infections can significantly improve the patient’s quality of life and potentially prolong their life.
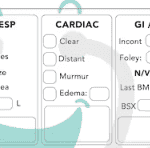
Hospice nurses play a vital role in providing quality care and comfort to terminally ill patients and their families. They must make accurate and timely assessments of the patient’s condition, needs, and preferences every visit. This article will outline the key aspects that hospice nurses should assess every visit, in addition to the standard physical assessment.
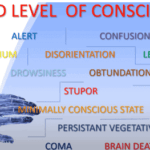
Understanding drowsiness, lethargy, and obtundation is crucial in hospice care. Drowsiness is a normal sleepiness, lethargy is more profound tiredness, and obtundation indicates severe unresponsiveness. Recognizing these levels helps in providing the right care and comfort for terminally ill patients.
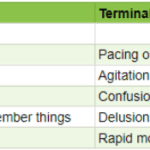
As an experienced hospice nurse, I understand how difficult it can be to distinguish between delirium and terminal restlessness. Both conditions can cause significant distress for the patient and their loved ones, and nurses must be able to tell the difference between them to provide the best possible care. In this article, I will share my knowledge and experience to help new hospice nurses understand the differences between delirium and terminal restlessness and how to rule out delirium.
Hospice care is focused on symptom management, pain relief, emotional support, and spiritual care. It is a privilege to be a part of a patient’s end-of-life journey, and as a new hospice nurse, you may feel overwhelmed, but you can make a difference in a patient’s life. One of the essential skills you need to learn as a hospice nurse is to recognize when to increase the scheduled visit frequency for a terminally ill patient under hospice care.

Terminal restlessness is a common phenomenon that occurs in the final stages of life. It is characterized by agitation, confusion, and distress. It can be challenging to recognize and manage, especially in patients who cannot communicate verbally. This article aims to share insights and tips from a hospice worker who learned how terminal restlessness can manifest differently in nonverbal patients and how to cope.

There are observation and interviewing skills you can develop which will help you learn:
What could cause the current change in condition
Determining if a patient is having terminal restlessness
Determining if your patient is within two weeks or less of life to live
Knowing where your patient is in the dying process
While this article is primarily meant for new nurses, what I’m sharing is also valuable for family members and loved ones. Anyone with patience and love toward the person being observed and interviewed can hone and develop these skills.
Falls among the elderly can have severe consequences, including hip fractures, which can be life-threatening. As an experienced hospice registered nurse case manager, I understand the importance of fall prevention, especially in private homes, personal care homes, and assisted living facilities. This article aims to provide practical tips for reducing falls in these settings by following the nursing process: assessment, diagnosis, planning, implementation, and evaluation.

Pain is a subjective sensation that can affect a person’s physical, emotional, and spiritual well-being. While pain can be measured objectively by using vital signs such as temperature, pulse, blood pressure, and respiration count, these indicators may not reflect the true intensity of pain that a person is experiencing. This is especially true for non-verbal patients, who cannot communicate their pain verbally. Non-verbal patients may include those with advanced dementia, terminal illness, or other conditions that impair their speech. In this article, I will discuss the importance of assessing pain in non-verbal patients, the tools and methods that can be used to do so, and the benefits of providing adequate pain relief for these patients.

When I first started working in the field of hospice, my clinical manager told me (I’m paraphrasing), one day you will be able to walk into the room, and without getting a single vital sign, just by visual observation, be able to tell that the person is dying or will be shortly dying. That was about three years ago. Today, it’s almost chilling for me (as it is both a blessing and tremendous responsibility) to be able to share she told the truth, and that over time — if you give yourself patience and grace and take the time to listen, observe, and remember — you too will learn how to tell when someone is close to or otherwise is dying.
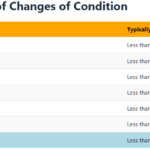
Please allow me to share some of my insight as to how I know a person has less than a month left to live, and often far less. First off, let’s go into the important discussion you should have with the family, friends, and the patient themselves that provides an overall background to the prognosis. That discussion should be centered around what types of decline (downward, negative) changes have been taking place in the patient’s life over the last six months making note as to whether the decline is minor, medium, or major and the frequency (once a month, once a week, etc.) of those changes.

Navigating the final days of a loved one's life can be a challenging and emotional journey. One of the signs that can be observed during this time is known as terminal restlessness. As someone deeply rooted in hospice care, I have witnessed various manifestations of this restlessness. Understanding its types, causes, and management strategies is crucial for providing compassionate end-of-life care. This article aims to illuminate the different kinds of terminal restlessness, identify reversible causes, and discuss effective management techniques. By equipping caregivers, families, and healthcare professionals with this knowledge, we can ensure that terminally ill individuals experience comfort and dignity in their final days.

If you are a new nurse to hospice, one of the tasks you probably dread is doing an admission especially if you have scheduled visits the same day as the admission.
I would like to share with you some tips that when applied may help lower your stress level, and help you remain on time even in cases where you have three to four visits including recertification to do the same day.