
Category: Tips and Tricks
Articles about tips and tricks for caregivers and nurses caring for the terminally ill.
Articles about tips and tricks for caregivers and nurses caring for the terminally ill.

Learn how to communicate effectively with healthcare professionals when caring for a loved one with a terminal illness. Improve communication, advocacy, and coping skills to ensure your loved one receives the best care possible.

Managing bowel problems in terminally ill patients is crucial for their comfort and dignity. This guide offers practical tips for caregivers and hospice nurses to address constipation, diarrhea, bowel obstruction, and ascites, ensuring patients' better quality of life.

Dementia is a complex condition affecting millions worldwide. Diagnosing dementia requires the expertise of medical professionals specializing in cognitive disorders. By guiding families and caregivers through the diagnostic process, you can empower them. In this article, we'll explore the steps to find the right specialist for a dementia diagnosis and how families can prepare for the crucial doctor visit.
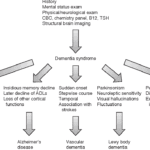
Getting a formal diagnosis of dementia is essential for understanding the condition, accessing appropriate treatments and support services, and ensuring the best possible care. This comprehensive guide explores the importance of a specific diagnosis in predicting patient needs for comfort and quality of life, as different types of dementia require distinct care approaches. Avoid the risks of a generic diagnosis and empower yourself with knowledge.

Caregivers can find it challenging to ensure dementia patients wear their CPAPs overnight. This article offers practical tips and strategies to help caregivers ensure comfortable and uninterrupted CPAP use for their loved ones.

This guide covers how to write effective hospice nursing narratives, key documentation areas, and the importance of detailed and negative-based wording to support continued hospice eligibility.

The journey towards the end of life can be a challenging and emotional time, both for the individual facing the end of their life and for their caregivers and family members. One aspect of this journey that may be unfamiliar to many is the presence of self-soothing sounds made by the patient during the transition and actively dying phase. These sounds can be puzzling and sometimes unsettling for caregivers and family members who have never witnessed them. This article will explore self-soothing sounds, why they occur, and how caregivers and family members can distinguish between self-soothing sounds and signs of discomfort.
This article delves into the intricate relationship between dementia and seizures, offering insights on identification, safety protocols, and advocacy for caregivers.

As a hospice admission nurse, asking the right questions is crucial for assessing patients' eligibility and providing compassionate care. This article explores critical questions to understand the patient's condition, decline timeline, hospitalizations, functional abilities, cognitive status, and comorbidities. By gathering this information, nurses can support informed decisions, tailor interventions, and ensure a "good death" for patients and families.
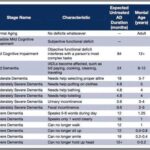
As a nurse who has cared for many terminally ill individuals with Alzheimer's disease over the years, I understand the importance of accurately assessing their functional decline using the Functional Assessment Staging Tool (FAST). The FAST scale provides valuable information about the progression of Alzheimer's disease and helps guide appropriate care planning for patients and their families. In this guide, I will walk you through the process of assessing patients on the FAST scale, starting from stage 1 and discussing when to stop reading the scale for determination. I will also provide three examples of patients at various stages of the FAST scale.
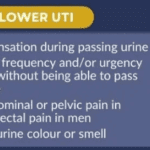
This comprehensive guide helps caregivers understand why urinary tract infections (UTIs) are prevalent in dementia patients. It provides practical advice on prevention, early detection, and effective treatment strategies. Empower yourself with the knowledge to provide the best care for your loved ones.

Discover essential time management strategies for hospice visiting nurses. Learn how to balance patient care, documentation, and self-care while navigating the unique challenges of rural hospice work. Improve your efficiency and effectiveness in providing compassionate end-of-life care.
Exploring Hospice Eligibility Criteria for Alzheimer's, Vascular, Lewy Body, Frontotemporal and other Dementias: Empowering Hospice Nurses to Provide Compassionate End-of-Life Care

This article is crafted with heartfelt understanding and care, recognizing the challenges you face as caregivers and family members of terminally ill loved ones. Our goal is to empower you with knowledge and practical advice to manage the risk of aspiration pneumonia, a common yet often preventable complication in hospice care.
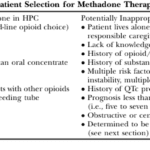
This article delves into the advantages of Methadone over Morphine for pain management in hospice settings. It covers dosage, titration, side effects, and scenarios where Methadone may not be the best choice. Ideal for hospice professionals and caregivers seeking compassionate pain relief options for the terminally ill.

Deciding on a dementia care facility is crucial. This guide compares personal care homes, assisted living, memory care units, and nursing facilities, detailing Medicaid eligibility, pros and cons, and essential questions to ensure the best care for your family member.

As a seasoned hospice nurse, I recognize the significance of adhering to Medicare guidelines to ensure top-notch patient care. Medicare guidelines offer a roadmap for hospice providers to offer exceptional care to terminally ill patients and their loved ones. Nonetheless, upholding compliance with these guidelines can be a hurdle, especially for smaller hospice providers with limited resources. In this article, we'll delve into how RN case managers can effectively ensure compliance with Medicare guidelines.
Uncover the importance of regular care plan meetings at healthcare facilities. This guide details participants, goals, benefits, and risks of non-participation.

If you or someone you love has a serious illness that cannot be cured, you may have heard of hospice care. Hospice care is a special kind that focuses on making the patient comfortable and peaceful in their final days. Hospice care also supports the family and caregivers emotionally and spiritually.
When a patient joins hospice care, they will have a special meeting with a hospice nurse. This meeting is called the post-admission visit. It is an especially important visit because it will help the patient and the family get to know the hospice team and learn more about the care they will receive.
This article will explain what to expect and what to ask during the post-admission visit. We will also provide tips and resources to help you and your loved one make the most of this time. We hope this article will help you feel more prepared and confident about the hospice journey.
Facing Creutzfeldt-Jakob Disease (CJD) can be overwhelming, but with the right information and compassionate care, you can navigate this journey with your loved one. This guide is designed to help families new to CJD understand what to expect, recognize changes in their loved one, and provide the best care from onset

Discover practical ways to show compassion in hospice care. Learn how small gestures like active listening, gentle touch, and respecting personal space can make a significant difference. Explore the importance of empathy, cultural sensitivity, and self-care for caregivers in providing compassionate end-of-life support.

Discover how Lion’s Mane, Magnesium Glycinate, Vitamins D3, K2, B1, Folate, C, and MTC Oil can play a role in dementia care. This article delves into the latest research and expert insights on natural supplements that support cognitive function and overall brain health.

Discover essential educational topics for hospice nurses during admission and follow-up visits. Learn how to effectively communicate with patients and families, manage symptoms, provide emotional support, and navigate end-of-life care. Enhance your skills to deliver compassionate, comprehensive hospice care.

Explore the use of ashwagandha and CBD to ease anxiety in dementia patients. Learn about dosages, safety precautions, and real-life stories.