
Category: Palliative Care
Articles about palliative care including the differences between palliative care and hospice care which is palliative care at end-of-life.
Articles about palliative care including the differences between palliative care and hospice care which is palliative care at end-of-life.

Deciding on a dementia care facility is crucial. This guide compares personal care homes, assisted living, memory care units, and nursing facilities, detailing Medicaid eligibility, pros and cons, and essential questions to ensure the best care for your family member.

As a seasoned hospice nurse, I recognize the significance of adhering to Medicare guidelines to ensure top-notch patient care. Medicare guidelines offer a roadmap for hospice providers to offer exceptional care to terminally ill patients and their loved ones. Nonetheless, upholding compliance with these guidelines can be a hurdle, especially for smaller hospice providers with limited resources. In this article, we'll delve into how RN case managers can effectively ensure compliance with Medicare guidelines.
Uncover the importance of regular care plan meetings at healthcare facilities. This guide details participants, goals, benefits, and risks of non-participation.
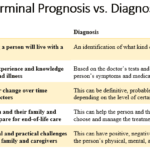
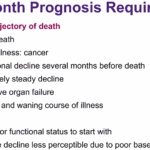
When a loved one is diagnosed with a terminal illness or a progressive disease, it can be a daunting and overwhelming experience for families and caregivers. Understanding the terms and concepts associated with these conditions is essential to providing the best possible care and support. This article aims to clarify the complex journey of terminal illnesses and progressive diseases, offering guidance and compassion to those navigating this challenging path.

Discover the essentials of Mild Cognitive Impairment (MCI) with our guide. Understand the signs, diagnosis, and ways to support loved ones facing the risk of dementia. This article provides valuable insights for patients, families, and caregivers to navigate the journey confidently.

If you or someone you love has a serious illness that cannot be cured, you may have heard of hospice care. Hospice care is a special kind that focuses on making the patient comfortable and peaceful in their final days. Hospice care also supports the family and caregivers emotionally and spiritually.
When a patient joins hospice care, they will have a special meeting with a hospice nurse. This meeting is called the post-admission visit. It is an especially important visit because it will help the patient and the family get to know the hospice team and learn more about the care they will receive.
This article will explain what to expect and what to ask during the post-admission visit. We will also provide tips and resources to help you and your loved one make the most of this time. We hope this article will help you feel more prepared and confident about the hospice journey.
Facing Creutzfeldt-Jakob Disease (CJD) can be overwhelming, but with the right information and compassionate care, you can navigate this journey with your loved one. This guide is designed to help families new to CJD understand what to expect, recognize changes in their loved one, and provide the best care from onset
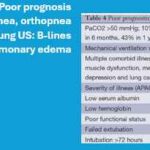
Dive into our in-depth analysis of CHF and COPD exacerbations. These critical events shape patient outcomes through expert insights and compelling case studies. Discover strategies for managing expectations and improving quality of life in the face of chronic illness.

If you or someone you love is facing a terminal illness, you may feel overwhelmed by the physical, emotional, and spiritual challenges that come with it. You may wonder how to cope with the pain, the fear, the grief, and the loss of control. You may also want to find ways to make the most of the time you have left and to leave a lasting legacy for your loved ones.
Music therapy is a form of therapy that can help you and your family deal with these issues. It involves using music and musical activities to improve the health and well-being of people of all ages and backgrounds. Music therapy can help you express your feelings, communicate with others, relax your body and mind, cope with pain and stress, enhance your spiritual connection, and create a meaningful life story.

Dive into the contrasting philosophies of purist and non-purist hospice nurses and doctors. Understand how their views on medication and patient care differ, shaping the terminal phase of a patient’s journey. This article highlights the delicate balance between medical intervention and quality of life in hospice care.
Discover practical ways to show compassion in hospice care. Learn how small gestures like active listening, gentle touch, and respecting personal space can make a significant difference. Explore the importance of empathy, cultural sensitivity, and self-care for caregivers in providing compassionate end-of-life support.
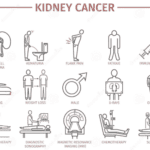
Receiving a diagnosis of kidney cancer for a beloved family member can be a challenging experience. However, by comprehending the stages of the disease and learning how to offer optimal care, you can help alleviate some of the overwhelming feelings associated with this journey. This article aims to empower you, a caring family member, with valuable insights. You will gain an understanding of the progression of kidney cancer, discover how to identify shifts in your loved one's condition, and learn how to provide exceptional care from the moment of diagnosis to the end-of-life phase.

Explore the profound journey of the actively dying. This article unravels the reasons behind their lingering, examining medical interventions and the emotional need for closure. Gain insight into this delicate phase of life."

Discover how Lion’s Mane, Magnesium Glycinate, Vitamins D3, K2, B1, Folate, C, and MTC Oil can play a role in dementia care. This article delves into the latest research and expert insights on natural supplements that support cognitive function and overall brain health.
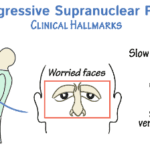
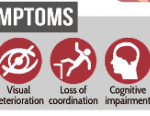
Navigating the complexities of end-stage Progressive Supranuclear Palsy can be challenging. Our comprehensive guide provides essential information, practical tips, and empathetic support to help families and caregivers through this difficult time.

Discover essential educational topics for hospice nurses during admission and follow-up visits. Learn how to effectively communicate with patients and families, manage symptoms, provide emotional support, and navigate end-of-life care. Enhance your skills to deliver compassionate, comprehensive hospice care.

Explore the use of ashwagandha and CBD to ease anxiety in dementia patients. Learn about dosages, safety precautions, and real-life stories.
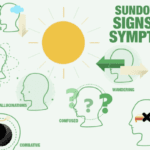
Sundowning, or "late-day confusion," is a challenging experience for individuals with dementia and their caregivers. This phenomenon, occurring in the late afternoon or evening, brings about increased confusion, anxiety, and agitation. Caregivers need to comprehend sundowning and offer compassionate care to ensure the well-being of their loved ones. This article delves into effective pharmacological and non-pharmacological strategies to manage sundowning and create a safe environment.
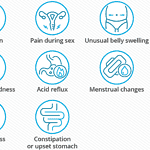
When a cherished family member receives an ovarian cancer diagnosis, the path ahead can feel daunting and complex. As a hospice registered nurse case manager specializing in empathetic end-of-life care, I am here to offer you clear and compassionate direction. In this article, we will discuss the anticipated stages of ovarian cancer, the transformations you may notice in your loved one, and effective methods to ensure optimal care from diagnosis to the journey's close.
Navigating the challenges of caring for an elderly parent with dementia can be tough, especially when they resist help. This guide offers practical advice and compassionate strategies to support your loved one while respecting their autonomy and dignity.

Discover the potential side effects of dementia medications and how to support your loved one. Stay informed!
Discover the true nature of hospice care in the U.S. This guide clarifies eligibility, focusing on comfort for those with a terminal prognosis of six months or less, and the support available for families and caregivers during this journey.

Maintaining routines and consistency can significantly improve the overall well-being and quality of life of a loved one with dementia. As a caregiver, understanding the value of routines and how they can positively impact your loved one's journey through dementia is crucial. In this article, we'll explore why routines matter, how to establish them, and their benefits to patients and caregivers.

An article that guides families through understanding and exercising their rights to choose the best hospice care for their loved ones, ensuring their final chapter is written with compassion and respect.