
Category: Palliative Care
Articles about palliative care including the differences between palliative care and hospice care which is palliative care at end-of-life.
Articles about palliative care including the differences between palliative care and hospice care which is palliative care at end-of-life.
When a loved one is terminally ill, it can be a perplexing and emotional journey. Understanding the root cause of their declining health becomes paramount. It's a complex puzzle where family members often grapple with questions: Are the symptoms a result of medications prescribed, or are they intrinsic to the terminal disease? This article delves into the critical distinctions between medication side effects and the natural progression of terminal illnesses, offering insights to empower families and caregivers in making informed decisions about their loved one's care.

Serotonin syndrome is a potentially life-threatening condition caused by an excess of serotonin in the body. Detecting this condition early is crucial, but it can be particularly challenging when dealing with dementia patients due to communication barriers and the complexity of their symptoms. In this article, we will present three case studies that highlight the early detection and successful management of serotonin syndrome in patients with different types of dementia: Alzheimer's disease, vascular dementia, and Lewy Body Dementia.

Hospice nurses assess the status of the patient's journey towards the end of life every nursing visit. Situations where a reversible condition can drastically impact the patient and the hospice assessment can occur. If it is not caught, it is potentially mistreated, leading to increased discomfort and a faster death, often involving increased suffering. One of the common clues that someone is getting closer to dying is increased agitation and restlessness.
Are you aware of Serotonin Syndrome?
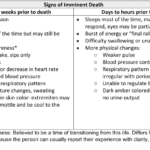
Discover key indicators for end-of-life care in hospice. This guide highlights ‘trigger words’ that signal a patient’s final days, aiding nurses and caregivers in providing compassionate support during the most critical moments.
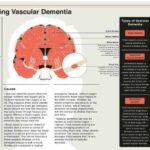
If your loved one has been diagnosed with Vascular Dementia, it is natural to have questions and concerns about what lies ahead. This educational article aims to provide you with an overview of what to expect over the course of the disease, the changes you might see in your loved one, and how to best care for them from onset until the end of life.

Hospice care is often misunderstood and shrouded in myths that can prevent individuals and families from accessing the compassionate support they need during a challenging time. This article will address common misconceptions about hospice care and provide you with the facts. We aim to empower you with accurate information to make informed decisions when considering hospice for yourself or a loved one.

Dementia is a condition that affects millions of people worldwide, and it can cause a range of symptoms, including pain and discomfort. Unfortunately, pain is often under-detected and undertreated in people with dementia, leading to significant suffering and a reduced quality of life. In this article, we will explore the prevalence of pain among dementia patients, the impact of unmanaged pain on their quality of life, behavioral changes that may indicate pain, and the use of the PAINAD pain scale as a tool for assessing and managing pain in dementia patients.
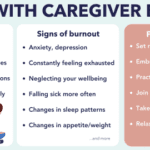
Caring for a loved one with dementia can be a rewarding experience, but it can also be physically, emotionally, and mentally exhausting. Family caregivers often neglect their own well-being while focusing on the needs of their loved ones, leading to burnout. Caregiver burnout is a state of physical, emotional, and mental exhaustion that can happen when caregivers don't get the help they need or try to do more than they are able to do. In this article, we will discuss how family caregivers of a loved one with dementia can avoid burnout and recover if they are already experiencing burnout.
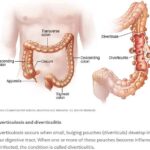
Caring for a loved one with a history of diverticulitis requires a combination of preventive measures, early detection of warning signs, and understanding the common signs and symptoms of this condition. Your role as a caregiver is crucial in providing support and assistance to ensure their well-being. In this comprehensive guide, we will explore essential aspects of caring for someone with diverticulitis, including prevention, early warning signs, and treatment options.
In the realm of hospice care, where empathy and compassion are paramount, a remarkable approach called Validation Therapy has emerged as a beacon of hope and comfort for individuals facing dementia and cognitive disorders in their final journey. As an experienced hospice registered nurse case manager, I've witnessed the transformative impact of Validation Therapy on patients, allowing them to find solace, regain their self-worth, and experience a sense of dignity during their end-of-life phase.
I understand how challenging it can be for terminally ill patients to cope with their fear of impending death. It is crucial for both healthcare providers and family members to take these feelings seriously and respond with compassion and understanding. In this article, we will explore the importance of acknowledging a patient's fear of impending doom and discuss actions that families can take to provide peace and comfort during this grim time.
Caring for individuals with dementia can be both challenging and rewarding. One approach that has gained recognition for promoting meaningful relationships with dementia patients is Validation Therapy, developed by Naomi Feil. This article will explore how Validation Therapy works, why it does not involve telling a single lie, and why honesty is crucial when dealing with dementia patients.
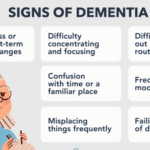
Dementia is a condition that affects cognitive abilities such as thinking, remembering, and reasoning. It is crucial to recognize the signs and symptoms of dementia early to provide proper support. This article will help you understand the common signs and symptoms of dementia and steps you can take to address them.

In this article, we will explore the vital role of a hospice chaplain, as explained by Katherine Seiler, an experienced and compassionate hospice chaplain. Hospice chaplains play a significant role in providing emotional, social, and spiritual support to terminally ill patients and their families during their end-of-life journey.

Facing a loved one's diagnosis of frontal lobe dementia can be overwhelming and challenging. This article aims to provide families with essential information about frontal lobe dementia, its progression, changes they might observe in their loved one, and best practices for caregiving from onset until the end of life.
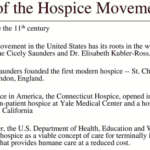
Hospice care is a vital form of healthcare dedicated to providing comfort and support to patients in their final stages of life. While it's a relatively recent concept in the United States, with its inception in 1974, it has gained significant popularity, with over half of Medicare beneficiaries in 2020 receiving hospice services. Nevertheless, as we delve into 2023, hospice care confronts several formidable challenges. These include labor shortages, concerns about the quality of care, and the notable presence of for-profit entities in the industry. In this article, we will navigate through the history of hospice care in the United States, its present state in 2023, and the challenges that affect not only hospice patients but also the dedicated staff and providers.
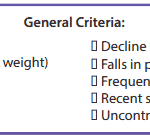
It’s essential to familiarize yourself with the key local coverage determination (LCD) facts for different terminal illnesses to avoid admitting patients who are not eligible for services only to be required to refund the money back to Medicare; otherwise, only have the patient on for one benefit period then discharged for failure to decline. These determinations provide guidelines on the coverage of hospice services for specific conditions. If you are the admitting nurse, please do not just admit because you were told to admit by someone, regardless of the position or standing of the person or party that told you to admit. Use your critical thinking and clinical judgment skills to evaluate the patient for admission. Most doctors will write "evaluate and treat" or something to that effect; never lose sight of the "evaluate" portion of the doctor's order.
Based on the provided PDF files, as noted in the resources section below, let’s explore some essential information for each terminal illness.
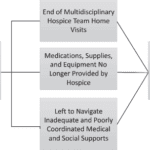
If your loved one is facing a discharge from hospice due to failure to decline, it's crucial to comprehend the situation clearly. This discharge indicates that the healthcare team believes your loved one's condition has stabilized and no longer requires hospice care. While this might be a positive sign, it's important to weigh the pros and cons before making decisions. Let's delve into both the positive and negative aspects of this situation to help you navigate it effectively.

Caring for a terminally ill loved one is a profound and challenging journey that requires compassion, understanding, and a willingness to alleviate any discomfort they may experience. In this guide, we will explore the concept of discomfort, its distinction from pain, and the importance of recognizing and addressing discomfort in addition to pain. You'll be better equipped to provide holistic care that enhances your loved one's quality of life during this sensitive time.
Throughout your loved one's illness, you might find yourself thinking that they don't require "pain medication" because they don't seem to be in pain. They might even respond with a direct "no" when asked about their pain. However, are you aware that most types of pain medication can alleviate discomfort? Did you also know that your loved one could be feeling uncomfortable without necessarily being in severe pain? Nonetheless, it's important to recognize that their discomfort requires the same treatment as if they were in pain.

As a family member of a terminally ill loved one receiving care in a facility, you play a vital role in ensuring they receive the best possible care and support during their journey towards a good death. Advocating for your loved one involves understanding their needs, communicating effectively with the facility staff, and staying informed about their care plan. This article aims to guide you on being an effective advocate, asking the right questions, and ensuring your loved one's comfort and well-being.

This article delves into hospice care with Andrew Viozzi, an adept hospice admission registered nurse. Andrew brings valuable insights into the hospice admission process and the broader spectrum of hospice care. Although Andrew's current position revolves around admissions, his extensive experience encompasses case management, preceptorship, mentorship, and the guidance of new hospice nurses. In this article, we dispel misconceptions, highlight the advantages of hospice care, outline the admission procedure, and emphasize the pivotal role of hospice in end-of-life care.
As an experienced hospice visiting registered nurse, today offered me profound insights from two interconnected perspectives. The first highlights the blind trust we often place in facility nurses and doctors when caring for our loved ones. The second involves the challenges I encountered while advocating for proper end-of-life care for a patient with Alzheimer's.

In the realm of hospice care, compassion and comfort take precedence. A team of skilled professionals comes together to offer comprehensive support to patients, their families, and caregivers. Among these essential contributors, Certified Nursing Assistants (CNAs) stand out as unsung heroes, bringing immeasurable value to the field of hospice care. This article delves into the distinctive role CNAs play in hospice, their frequent and meaningful interactions, and their leadership within the hospice team.
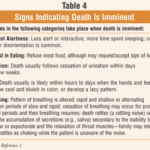
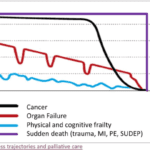
For a non-healthcare professional who has never witnessed death before, it can be unsettling to be present with someone who is nearing the end of their life. However, there are certain signs and observations that you can make using your senses that may indicate that the person you are with may pass away within seconds, minutes, or hours. Understanding these signs can help you provide support and comfort to the individual and their loved ones during this grim time.