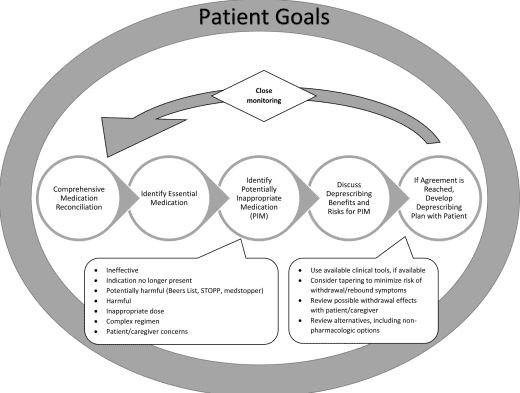
Medication reconciliation and deprescribing are two important processes that can improve the quality of care and safety of hospice patients. Medication reconciliation is the process of creating and maintaining an accurate and complete list of all the medications that a patient is taking, including the dose, frequency, route, and indication. Deprescribing is the process of reducing or stopping medications that are no longer beneficial, necessary, or appropriate for the patient’s condition and goals of care.
Medication reconciliation and deprescribing are especially important for terminally ill hospice patients, who often have multiple chronic conditions, complex medication regimens, and limited life expectancy. These patients may be exposed to potentially inappropriate medications (PIMs) that can cause adverse effects, drug interactions, and increased burden and cost. PIMs are medications that have more risks than benefits for a specific patient or population, or that are not aligned with the patient’s preferences and values. By identifying and avoiding PIMs, medication reconciliation and deprescribing can help hospice patients achieve better symptom control, comfort, and quality of life.
One of the tools that can help healthcare providers perform medication reconciliation and deprescribing for hospice patients is the Beers Criteria for Potentially Inappropriate Medication Use in Older Adults, commonly known as the Beers Criteria or the Beers List. The Beers Criteria is a list of medications that are best avoided or used with caution by older adults (65 years and older) in most circumstances or under specific situations, such as certain diseases, conditions, or care settings. The Beers Criteria is developed and updated by the American Geriatrics Society (AGS) based on the best available evidence and expert consensus. The Beers Criteria can serve as a guide for healthcare providers to improve medication selection, educate patients and caregivers, and evaluate quality of care, cost, and patterns of drug use in older adults.
In this article, we will discuss how to use the Beers Criteria to identify PIMs and potential prescribing omissions (PPOs) in hospice patients. PPOs are medications that are indicated but not prescribed for a specific patient or population, or that are prescribed at a suboptimal dose or duration. We will also present 10 case studies to illustrate the medication reconciliation and deprescribing process and the outcomes of medication changes in different scenarios.
We hope that these case studies will help you to improve your medication management skills and provide better care for your hospice patients. Let’s get started!
Case Study 1: A 78-year-old woman with advanced ovarian cancer and multiple comorbidities
Meet Mrs. A, a 78-year-old woman who was admitted to hospice care with advanced ovarian cancer and multiple comorbidities, including hypertension, diabetes, osteoporosis, and depression. She has a prognosis of less than 6 months to live, and her main goal of care is to be comfortable and pain-free.
Her current medication list includes:
Morphine sulfate 30 mg orally every 4 hours as needed for pain
Ondansetron 8 mg orally twice daily for nausea
Dexamethasone 4 mg orally once daily for appetite stimulation
Metformin 500 mg orally twice daily for diabetes
Lisinopril 10 mg orally once daily for hypertension
Amlodipine 5 mg orally once daily for hypertension
Alendronate 70 mg orally once weekly for osteoporosis
Calcium carbonate 500 mg orally twice daily for osteoporosis
Vitamin D3 1000 IU orally once daily for osteoporosis
Sertraline 50 mg orally once daily for depression
To apply the Beers criteria to Mrs. A’s medication list, we need to review each medication and compare it with the relevant indicators for her condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Morphine sulfate
No specific criteria
Appropriate
Opioids are indicated for moderate to severe pain in palliative care
Ondansetron
No specific criteria
Appropriate
Antiemetics are indicated for nausea and vomiting in palliative care
Dexamethasone
No specific criteria
Appropriate
Corticosteroids are indicated for appetite stimulation and symptom control in palliative care
Metformin
Avoid in patients with renal impairment (eGFR < 30 mL/min/1.73 m2)
PIM
Metformin may cause lactic acidosis and hypoglycemia in patients with renal failure
Lisinopril
Avoid in patients with renal impairment (eGFR < 30 mL/min/1.73 m2)
PIM
Lisinopril may cause hyperkalemia, renal impairment, and angioedema in patients with renal failure
Amlodipine
No specific criteria
Appropriate
Calcium channel blockers are indicated for hypertension in renal failure
Alendronate
Avoid in patients with life expectancy < 1 year
PIM
Alendronate may cause esophagitis, osteonecrosis of the jaw, and atypical fractures in patients with short life expectancy
Calcium carbonate
Avoid in patients with hypercalcemia or renal impairment (eGFR < 30 mL/min/1.73 m2)
PIM
Calcium carbonate may cause hypercalcemia, constipation, and drug interactions in patients with renal failure
Vitamin D3
Avoid in patients with hypercalcemia or renal impairment (eGFR < 30 mL/min/1.73 m2)
PIM
Vitamin D3 may cause hypercalcemia, vascular calcification, and drug interactions in patients with renal failure
Sertraline
Avoid in patients with hyponatremia or bleeding risk
PIM
Sertraline may cause hyponatremia, bleeding, and drug interactions in patients with renal failure or anticoagulant use
Based on the table, we can see that Mrs. A has 6 PIMs in her medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mrs. A about her pain, nausea, appetite, blood glucose, blood pressure, calcium, and any other concerns. Ask her about her expectations and preferences regarding her medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mrs. A, we can prioritize the medications as follows:
High priority: Metformin, lisinopril, alendronate, calcium carbonate, vitamin D3, sertraline. These medications have an elevated risk of harm and low benefit for Mrs. A. They can be stopped immediately without tapering.
Medium priority: None. All other medications are appropriate for Mrs. A’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mrs. A’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mrs. A are as follows:
After stopping metformin, lisinopril, alendronate, calcium carbonate, vitamin D3, and sertraline, her blood glucose, blood pressure, calcium, and bleeding risk stabilized and she did not experience any lactic acidosis, hypoglycemia, hyperkalemia, renal impairment, angioedema, esophagitis, osteonecrosis of the jaw, atypical fractures, hypercalcemia, constipation, vascular calcification, hyponatremia, or drug interactions. She also reported less depression and anxiety.
After continuing morphine, ondansetron, dexamethasone, and amlodipine, her pain, nausea, appetite, and blood pressure remained well controlled. She did not experience any adverse effects from these medications.
Mrs. A was satisfied with the deprescribing process and felt more comfortable and confident with her medication regimen. She expressed gratitude to the hospice team for their care and support. She died peacefully at home a few months later.
Case Study 2: A 65-year-old man with end-stage chronic obstructive pulmonary disease and severe anxiety
Meet Mr. B, a 65-year-old man who was admitted to hospice care with end-stage chronic obstructive pulmonary disease (COPD) and severe anxiety. He has a prognosis of less than 6 months to live, and his main goal of care is to breathe easier and reduce his anxiety.
His current medication list includes:
Albuterol inhaler 2 puffs every 4 hours as needed for shortness of breath
Budesonide/formoterol inhaler 2 puffs twice daily for COPD maintenance
Tiotropium inhaler 1 puff once daily for COPD maintenance
Prednisone 10 mg orally once daily for COPD exacerbation
Lorazepam 1 mg orally every 6 hours as needed for anxiety
Paroxetine 20 mg orally once daily for anxiety
Acetaminophen 500 mg orally every 6 hours as needed for pain
Omeprazole 20 mg orally once daily for gastroesophageal reflux disease (GERD)
To apply the Beers criteria to Mr. B’s medication list, we need to review each medication and compare it with the relevant indicators for his condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Albuterol
No specific criteria
Appropriate
Short-acting beta-agonists are indicated for acute bronchospasm in COPD
Budesonide/formoterol
No specific criteria
Appropriate
Long-acting beta-agonists and inhaled corticosteroids are indicated for COPD maintenance in patients with frequent exacerbations
Tiotropium
No specific criteria
Appropriate
Long-acting anticholinergics are indicated for COPD maintenance in patients with frequent exacerbations
Prednisone
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Prednisone may cause delirium, psychosis, insomnia, and hyperglycemia in patients with cognitive impairment
Lorazepam
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Lorazepam may cause sedation, confusion, falls, dependence, and withdrawal in patients with cognitive impairment
Paroxetine
Avoid in patients with hyponatremia or bleeding risk
PIM
Paroxetine may cause hyponatremia, bleeding, and drug interactions in patients with renal failure or anticoagulant use
Acetaminophen
No specific criteria
Appropriate
Acetaminophen is a safe and effective analgesic for mild to moderate pain
Omeprazole
Avoid in patients with life expectancy < 1 year
PIM
Omeprazole may cause hypomagnesemia, osteoporosis, infections, and rebound acid hypersecretion in patients with short life expectancy
Based on the table, we can see that Mr. B has 3 PIMs in his medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mr. B about his shortness of breath, anxiety, pain, reflux, blood glucose, and any other concerns. Ask him about his expectations and preferences regarding his medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mr. B, we can prioritize the medications as follows:
High priority: Prednisone, lorazepam, paroxetine, omeprazole. These medications have an elevated risk of harm and low benefit for Mr. B. They can be tapered gradually over a few weeks or months to avoid withdrawal symptoms and worsening anxiety or depression.
Medium priority: None. All other medications are appropriate for Mr. B’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mr. B’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mr. B are as follows:
After tapering prednisone, lorazepam, paroxetine, and omeprazole, his delirium, psychosis, insomnia, hyperglycemia, sedation, confusion, falls, dependence, withdrawal, hyponatremia, bleeding, and drug interactions improved, and he did not experience any worsening of his COPD or anxiety. He also reported less reflux and heartburn.
After continuing albuterol, budesonide/formoterol, tiotropium, acetaminophen, and morphine, his shortness of breath, COPD exacerbations, and pain remained well controlled. He did not experience any adverse effects from these medications.
Mr. B was satisfied with the deprescribing process and felt more comfortable and confident with his medication regimen. He expressed gratitude to the hospice team for their care and support. He died peacefully at home a few months later.
Case Study 3: A 72-year-old woman with metastatic breast cancer and refractory pain
Meet Mrs. C, a 72-year-old woman who was admitted to hospice care with metastatic breast cancer and refractory pain. She has a prognosis of less than 6 months to live, and her main goal of care is to relieve her pain and suffering.
Her current medication list includes:
Hydromorphone 4 mg orally every 4 hours as needed for breakthrough pain
Fentanyl patch 100 mcg/hour applied every 72 hours for baseline pain
Gabapentin 300 mg orally three times daily for neuropathic pain
Ibuprofen 400 mg orally every 6 hours as needed for inflammatory pain
Docusate sodium 100 mg orally twice daily for constipation
Senna 8.6 mg orally twice daily for constipation
Metoclopramide 10 mg orally four times daily for nausea
Haloperidol 0.5 mg orally every 6 hours as needed for nausea
Tamoxifen 20 mg orally once daily for hormone receptor-positive breast cancer
Letrozole 2.5 mg orally once daily for hormone receptor-positive breast cancer
To apply the Beers criteria to Mrs. C’s medication list, we need to review each medication and compare it with the relevant indicators for her condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Hydromorphone
No specific criteria
Appropriate
Opioids are indicated for moderate to severe pain in palliative care
Fentanyl patch
No specific criteria
Appropriate
Opioids are indicated for moderate to severe pain in palliative care
Gabapentin
Avoid in patients with renal impairment (eGFR < 30 mL/min/1.73 m2)
PIM
Gabapentin may cause sedation, dizziness, and edema in patients with renal failure
Ibuprofen
Avoid in patients with history of peptic ulcer disease or gastrointestinal bleeding
PIM
Ibuprofen may cause peptic ulcer, gastrointestinal bleeding, renal impairment, and fluid retention in patients with gastrointestinal risk factors
Docusate sodium
No specific criteria
Appropriate
Stool softeners are indicated for constipation in palliative care
Senna
No specific criteria
Appropriate
Stimulant laxatives are indicated for constipation in palliative care
Metoclopramide
Avoid in patients with Parkinson’s disease or extrapyramidal symptoms
PIM
Metoclopramide may cause extrapyramidal symptoms, tardive dyskinesia, and sedation in patients with neurological risk factors
Haloperidol
Avoid in patients with Parkinson’s disease or extrapyramidal symptoms
PIM
Haloperidol may cause extrapyramidal symptoms, tardive dyskinesia, and sedation in patients with neurological risk factors
Tamoxifen
Avoid in patients with life expectancy < 1 year
PIM
Tamoxifen may cause hot flashes, vaginal bleeding, and thromboembolism in patients with short life expectancy
Letrozole
Avoid in patients with life expectancy < 1 year
PIM
Letrozole may cause hot flashes, arthralgia, and osteoporosis in patients with short life expectancy
Based on the table, we can see that Mrs. C has 6 PIMs in her medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mrs. C about her pain, nausea, constipation, breast cancer, and any other concerns. Ask her about her expectations and preferences regarding her medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mrs. C, we can prioritize the medications as follows:
High priority: Gabapentin, ibuprofen, metoclopramide, haloperidol, tamoxifen, letrozole. These medications have an elevated risk of harm and low benefit for Mrs. C. They can be stopped immediately without tapering.
Medium priority: None. All other medications are appropriate for Mrs. C’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mrs. C’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mrs. C are as follows:
After stopping gabapentin, ibuprofen, metoclopramide, haloperidol, tamoxifen, and letrozole, her pain, nausea, constipation, and breast cancer remained well controlled and she did not experience any sedation, dizziness, edema, peptic ulcer, gastrointestinal bleeding, renal impairment, fluid retention, extrapyramidal symptoms, tardive dyskinesia, hot flashes, vaginal bleeding, thromboembolism, arthralgia, or osteoporosis. She also reported less anxiety and depression.
After continuing hydromorphone, fentanyl, docusate, senna, and acetaminophen, her pain and constipation remained well controlled. She did not experience any adverse effects from these medications.
Mrs. C was satisfied with the deprescribing process and felt more comfortable and confident with her medication regimen. She expressed gratitude to the hospice team for their care and support. She died peacefully at home a few months later.
Case Study 4: A 84-year-old man with advanced dementia and recurrent urinary tract infections
Meet Mr. D, a 84-year-old man who was admitted to hospice care with advanced dementia and recurrent urinary tract infections (UTIs). He has a prognosis of less than 6 months to live, and his main goal of care is to be comfortable and free of infections.
His current medication list includes:
Memantine 10 mg orally twice daily for dementia
Donepezil 10 mg orally once daily for dementia
Citalopram 20 mg orally once daily for depression
Lorazepam 0.5 mg orally every 6 hours as needed for agitation
Acetaminophen 500 mg orally every 6 hours as needed for pain
Nitrofurantoin 100 mg orally twice daily for UTI prophylaxis
Cranberry extract 500 mg orally once daily for UTI prevention
Multivitamin tablet orally once daily for general health
To apply the Beers criteria to Mr. D’s medication list, we need to review each medication and compare it with the relevant indicators for his condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Memantine
No specific criteria
Appropriate
NMDA receptor antagonists are indicated for moderate to severe dementia
Donepezil
No specific criteria
Appropriate
Cholinesterase inhibitors are indicated for mild to moderate dementia
Citalopram
Avoid in patients with QT interval prolongation or heart failure
PIM
Citalopram may cause QT interval prolongation, torsades de pointes, and cardiac arrhythmias in patients with cardiac risk factors
Lorazepam
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Lorazepam may cause sedation, confusion, falls, dependence, and withdrawal in patients with cognitive impairment
Acetaminophen
No specific criteria
Appropriate
Acetaminophen is a safe and effective analgesic for mild to moderate pain
Nitrofurantoin
Avoid in patients with renal impairment (CrCl < 30 mL/min) or chronic pulmonary disease
PIM
Nitrofurantoin may cause pulmonary toxicity, hepatotoxicity, and peripheral neuropathy in patients with renal or pulmonary impairment
Cranberry extract
No specific criteria
Appropriate
Cranberry extract may prevent UTIs by inhibiting bacterial adhesion to the urinary tract
Multivitamin tablet
No specific criteria
Appropriate
Multivitamin supplements may provide essential nutrients for general health
Based on the table, we can see that Mr. D has 2 PIMs in his medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mr. D about his dementia, depression, agitation, pain, UTIs, and any other concerns. Ask him about his expectations and preferences regarding his medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mr. D, we can prioritize the medications as follows:
High priority: Citalopram, lorazepam, nitrofurantoin. These medications have elevated risk of harm and low benefit for Mr. D. They can be tapered gradually over a few weeks or months to avoid withdrawal symptoms and worsening of depression or agitation.
Medium priority: None. All other medications are appropriate for Mr. D’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mr. D’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mr. D are as follows:
After tapering citalopram, lorazepam, and nitrofurantoin, his dementia, depression, agitation, pain, and UTIs remained well controlled and he did not experience any QT interval prolongation, torsade’s de pointes, cardiac arrhythmias, sedation, confusion, falls, dependence, withdrawal, pulmonary toxicity, hepatotoxicity, or peripheral neuropathy. He also reported less anxiety and restlessness.
After continuing memantine, donepezil, acetaminophen, cranberry extract, and multivitamin tablet, his dementia, pain, UTI prevention, and general health remained well maintained. He did not experience any adverse effects from these medications.
Mr. D was satisfied with the deprescribing process and felt more comfortable and confident with his medication regimen. He expressed gratitude to the hospice team for their care and support. He died peacefully at home a few months later.
Case Study 5: A 69-year-old woman with end-stage heart failure and depression
Meet Mrs. E, a 69-year-old woman who was admitted to hospice care with end-stage heart failure and depression. She has a prognosis of less than 6 months to live, and her main goal of care is to improve her mood and quality of life.
Her current medication list includes:
Furosemide 40 mg orally twice daily for fluid retention
Spironolactone 25 mg orally once daily for fluid retention
Carvedilol 12.5 mg orally twice daily for heart failure
Lisinopril 10 mg orally once daily for heart failure
Digoxin 0.125 mg orally once daily for heart failure
Warfarin 5 mg orally once daily for atrial fibrillation
Escitalopram 10 mg orally once daily for depression
Mirtazapine 15 mg orally once daily for depression
Lorazepam 0.5 mg orally every 6 hours as needed for anxiety
Morphine sulfate 10 mg orally every 4 hours as needed for dyspnea
To apply the Beers criteria to Mrs. E’s medication list, we need to review each medication and compare it with the relevant indicators for her condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Furosemide
No specific criteria
Appropriate
Loop diuretics are indicated for fluid retention in heart failure
Spironolactone
No specific criteria
Appropriate
Aldosterone antagonists are indicated for fluid retention in heart failure
Carvedilol
No specific criteria
Appropriate
Beta-blockers are indicated for heart failure and atrial fibrillation
Lisinopril
No specific criteria
Appropriate
ACE inhibitors are indicated for heart failure and hypertension
Digoxin
Avoid in patients with renal impairment (eGFR < 30 mL/min/1.73 m2) or life expectancy < 1 year
PIM
Digoxin may cause toxicity, arrhythmias, and increased mortality in patients with renal failure or short life expectancy
Warfarin
Avoid in patients with bleeding risk or life expectancy < 1 year
PIM
Warfarin may cause bleeding, bruising, and drug interactions in patients with bleeding risk factors or short life expectancy
Escitalopram
Avoid in patients with QT interval prolongation or heart failure
PIM
Escitalopram may cause QT interval prolongation, torsades de pointes, and cardiac arrhythmias in patients with cardiac risk factors
Mirtazapine
Avoid in patients with hyponatremia or bleeding risk
PIM
Mirtazapine may cause hyponatremia, bleeding, and drug interactions in patients with renal failure or anticoagulant use
Lorazepam
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Lorazepam may cause sedation, confusion, falls, dependence, and withdrawal in patients with cognitive impairment
Morphine sulfate
No specific criteria
Appropriate
Opioids are indicated for dyspnea and pain in palliative care
Based on the table, we can see that Mrs. E has 5 PIMs in her medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mrs. E about her dyspnea, fluid retention, heart failure, atrial fibrillation, depression, anxiety, pain, and any other concerns. Ask her about her expectations and preferences regarding her medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mrs. E, we can prioritize the medications as follows:
High priority: Digoxin, warfarin, escitalopram, mirtazapine, lorazepam. These medications have elevated risk of harm and low benefit for Mrs. E. They can be tapered gradually over a few weeks or months to avoid withdrawal symptoms and worsening of heart failure or depression.
Medium priority: None. All other medications are appropriate for Mrs. E’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mrs. E’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mrs. E are as follows:
After tapering digoxin, warfarin, escitalopram, mirtazapine, and lorazepam, her dyspnea, fluid retention, heart failure, atrial fibrillation, depression, anxiety, and pain remained well controlled and she did not experience any toxicity, arrhythmias, increased mortality, bleeding, bruising, drug interactions, QT interval prolongation, torsades de pointes, cardiac arrhythmias, hyponatremia, sedation, confusion, falls, dependence, or withdrawal. She also reported more energy and appetite.
After continuing furosemide, spironolactone, carvedilol, lisinopril, and morphine, her dyspnea, fluid retention, heart failure, atrial fibrillation, and pain remained well controlled. She did not experience any adverse effects from these medications.
Mrs. E was satisfied with the deprescribing process and felt more comfortable and confident with her medication regimen. She expressed gratitude to the hospice team for their care and support. She died peacefully at home a few months later.
Case Study 6: A 76-year-old man with amyotrophic lateral sclerosis and dysphagia
Meet Mr. F, a 76-year-old man who was admitted to hospice care with amyotrophic lateral sclerosis (ALS) and dysphagia. He has a prognosis of less than 6 months to live, and his main goal of care is to maintain his dignity and comfort.
His current medication list includes:
Riluzole 50 mg orally twice daily for ALS
Baclofen 10 mg orally three times daily for spasticity
Diazepam 5 mg orally every 6 hours as needed for anxiety
Amitriptyline 25 mg orally once daily for depression
Morphine sulfate 10 mg orally every 4 hours as needed for pain
Omeprazole 20 mg orally once daily for gastroesophageal reflux disease (GERD)
Polyethylene glycol 3350 17 g orally once daily for constipation
Senna 8.6 mg orally twice daily for constipation
To apply the Beers criteria to Mr. F’s medication list, we need to review each medication and compare it with the relevant indicators for his condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Riluzole
No specific criteria
Appropriate
Glutamate receptor antagonists are indicated for ALS
Baclofen
No specific criteria
Appropriate
Muscle relaxants are indicated for spasticity in ALS
Diazepam
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Benzodiazepines may cause sedation, confusion, falls, dependence, and withdrawal in patients with cognitive impairment
Amitriptyline
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Tricyclic antidepressants may cause anticholinergic effects, orthostatic hypotension, sedation, confusion, falls, and cardiac arrhythmias in patients with cognitive impairment
Morphine sulfate
No specific criteria
Appropriate
Opioids are indicated for pain and dyspnea in palliative care
Omeprazole
Avoid in patients with life expectancy < 1 year
PIM
Proton pump inhibitors may cause hypomagnesemia, osteoporosis, infections, and rebound acid hypersecretion in patients with short life expectancy
Polyethylene glycol 3350
No specific criteria
Appropriate
Osmotic laxatives are indicated for constipation in palliative care
Senna
No specific criteria
Appropriate
Stimulant laxatives are indicated for constipation in palliative care
Based on the table, we can see that Mr. F has 3 PIMs in his medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mr. F about his ALS, spasticity, anxiety, depression, pain, dyspnea, reflux, constipation, and any other concerns. Ask him about his expectations and preferences regarding his medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mr. F, we can prioritize the medications as follows:
High priority: Diazepam, amitriptyline, omeprazole. These medications have an elevated risk of harm and low benefit for Mr. F. They can be tapered gradually over a few weeks or months to avoid withdrawal symptoms and worsening of anxiety or depression.
Medium priority: None. All other medications are appropriate for Mr. F’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mr. F’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mr. F are as follows:
After tapering diazepam, amitriptyline, and omeprazole, his ALS, spasticity, pain, dyspnea, reflux, and constipation remained well controlled and he did not experience any sedation, confusion, falls, dependence, withdrawal, anticholinergic effects, orthostatic hypotension, cardiac arrhythmias, hypomagnesemia, osteoporosis, infections, or rebound acid hypersecretion. He also reported more alertness and mood improvement.
After continuing riluzole, baclofen, morphine, polyethylene glycol, and senna, his ALS, spasticity, pain, dyspnea, and constipation remained well controlled. He did not experience any adverse effects from these medications.
Mr. F was satisfied with the deprescribing process and felt more comfortable and confident with his medication regimen. He expressed gratitude to the hospice team for their care and support. He died peacefully at home a few months later.
Case Study 7: A 82-year-old woman with Parkinson’s disease and psychosis
Meet Mrs. G, a 82-year-old woman who was admitted to hospice care with Parkinson’s disease and psychosis. She has a prognosis of less than 6 months to live, and her main goal of care is to reduce her hallucinations and agitation.
Her current medication list includes:
Levodopa/carbidopa 100/25 mg orally three times daily for Parkinson’s disease
Pramipexole 0.5 mg orally three times daily for Parkinson’s disease
Amantadine 100 mg orally twice daily for Parkinson’s disease
Quetiapine 25 mg orally twice daily for psychosis
Lorazepam 0.5 mg orally every 6 hours as needed for agitation
Paroxetine 20 mg orally once daily for depression
Acetaminophen 500 mg orally every 6 hours as needed for pain
Bisacodyl 10 mg rectally once daily for constipation
To apply the Beers criteria to Mrs. G’s medication list, we need to review each medication and compare it with the relevant indicators for her condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Levodopa/carbidopa
No specific criteria
Appropriate
Dopamine precursors are indicated for Parkinson’s disease
Pramipexole
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Dopamine agonists may cause hallucinations, confusion, impulse control disorders, and orthostatic hypotension in patients with cognitive impairment
Amantadine
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
NMDA receptor antagonists may cause confusion, hallucinations, and anticholinergic effects in patients with cognitive impairment
Quetiapine
Avoid in patients with Parkinson’s disease or extrapyramidal symptoms
PIM
Atypical antipsychotics may worsen motor function and increase mortality in patients with Parkinson’s disease
Lorazepam
Avoid in patients with delirium, dementia, or cognitive impairment
PIM
Benzodiazepines may cause sedation, confusion, falls, dependence, and withdrawal in patients with cognitive impairment
Paroxetine
Avoid in patients with hyponatremia or bleeding risk
PIM
Selective serotonin reuptake inhibitors may cause hyponatremia, bleeding, and drug interactions in patients with renal failure or anticoagulant use
Acetaminophen
No specific criteria
Appropriate
Acetaminophen is a safe and effective analgesic for mild to moderate pain
Bisacodyl
No specific criteria
Appropriate
Stimulant laxatives are indicated for constipation in palliative care
Based on the table, we can see that Mrs. G has 5 PIMs in her medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mrs. G about her Parkinson’s disease, psychosis, agitation, depression, pain, constipation, and any other concerns. Ask her about her expectations and preferences regarding her medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mrs. G, we can prioritize the medications as follows:
High priority: Pramipexole, amantadine, quetiapine, lorazepam, paroxetine. These medications have an elevated risk of harm and low benefit for Mrs. G. They can be tapered gradually over a few weeks or months to avoid withdrawal symptoms and worsening of psychosis or depression.
Medium priority: None. All other medications are appropriate for Mrs. G’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mrs. G’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mrs. G are as follows:
After tapering pramipexole, amantadine, quetiapine, lorazepam, and paroxetine, her Parkinson’s disease, psychosis, agitation, depression, pain, and constipation remained well controlled and she did not experience any hallucinations, confusion, impulse control disorders, orthostatic hypotension, anticholinergic effects, worsening of motor function, increased mortality, sedation, falls, dependence, withdrawal, hyponatremia, bleeding, or drug interactions. She also reported more clarity and calmness.
After continuing levodopa/carbidopa, acetaminophen, and bisacodyl, her Parkinson’s disease, pain, and constipation remained well controlled. She did not experience any adverse effects from these medications.
Mrs. G was satisfied with the deprescribing process and felt more comfortable and confident with her medication regimen. She expressed gratitude to the hospice team for their care and support. She died peacefully at home a few months later.
Case Study 8: A 74-year-old man with prostate cancer and bone metastases
Meet Mr. H, a 74-year-old man who was admitted to hospice care with prostate cancer and bone metastases. He has a prognosis of less than 6 months to live, and his main goal of care is to reduce his pain and fatigue.
His current medication list includes:
Bicalutamide 50 mg orally once daily for prostate cancer
Leuprolide 22.5 mg intramuscularly every 3 months for prostate cancer
Zoledronic acid 4 mg intravenously every 4 weeks for bone metastases
Morphine sulfate 30 mg orally every 4 hours as needed for pain
Ibuprofen 400 mg orally every 6 hours as needed for pain
Ondansetron 8 mg orally twice daily for nausea
Dexamethasone 4 mg orally once daily for appetite stimulation
Ferrous sulfate 325 mg orally once daily for anemia
Folic acid 1 mg orally once daily for anemia
Cyanocobalamin 1000 mcg intramuscularly once a month for anemia
To apply the Beers criteria to Mr. H’s medication list, we need to review each medication and compare it with the relevant indicators for his condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Bicalutamide
No specific criteria
Appropriate
Antiandrogens are indicated for prostate cancer
Leuprolide
No specific criteria
Appropriate
Gonadotropin-releasing hormone agonists are indicated for prostate cancer
Zoledronic acid
No specific criteria
Appropriate
Bisphosphonates are indicated for bone metastases
Morphine sulfate
No specific criteria
Appropriate
Opioids are indicated for moderate to severe pain in palliative care
Ibuprofen
Avoid in patients with history of peptic ulcer disease or gastrointestinal bleeding
PIM
Nonsteroidal anti-inflammatory drugs may cause peptic ulcer, gastrointestinal bleeding, renal impairment, and fluid retention in patients with gastrointestinal risk factors
Ondansetron
No specific criteria
Appropriate
Serotonin receptor antagonists are indicated for nausea and vomiting in palliative care
Dexamethasone
No specific criteria
Appropriate
Corticosteroids are indicated for appetite stimulation and symptom control in palliative care
Ferrous sulfate
Avoid in patients with life expectancy < 1 year
PIM
Iron supplements may cause constipation, nausea, and drug interactions in patients with short life expectancy
Folic acid
Avoid in patients with life expectancy < 1 year
PIM
Folic acid supplements may cause masking of vitamin B12 deficiency, nausea, and drug interactions in patients with short life expectancy
Cyanocobalamin
Avoid in patients with life expectancy < 1 year
PIM
Vitamin B12 supplements may cause hypokalemia, thrombosis, and drug interactions in patients with short life expectancy
Based on the table, we can see that Mr. H has 4 PIMs in his medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mr. H about his prostate cancer, bone metastases, pain, nausea, appetite, anemia, and any other concerns. Ask him about his expectations and preferences regarding his medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mr. H, we can prioritize the medications as follows:
High priority: Ibuprofen, ferrous sulfate, folic acid, cyanocobalamin. These medications have an elevated risk of harm and low benefit for Mr. H. They can be stopped immediately without tapering.
Medium priority: None. All other medications are appropriate for Mr. H’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mr. H’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mr. H are as follows:
After stopping ibuprofen, ferrous sulfate, folic acid, and cyanocobalamin, his prostate cancer, bone metastases, pain, nausea, appetite, and anemia remained well controlled and he did not experience any peptic ulcer, gastrointestinal bleeding, renal impairment, fluid retention, constipation, nausea, drug interactions, masking of vitamin B12 deficiency, hypokalemia, thrombosis, or drug interactions. He also reported less fatigue and weakness.
After continuing bicalutamide, leuprolide, zoledronic acid, morphine, ondansetron, and dexamethasone, his prostate cancer, bone metastases, pain, nausea, and appetite remained well controlled. He did not experience any adverse effects from these medications.
Mr. H was satisfied with the deprescribing process and felt more comfortable and confident with his medication regimen. He expressed gratitude to the hospice team for their care and support. He died peacefully at home a few months later.
Case Study 9: A 68-year-old woman with liver cirrhosis and ascites
Meet Mrs. I, a 68-year-old woman who was admitted to hospice care with liver cirrhosis and ascites. She has a prognosis of less than 6 months to live, and her main goal of care is to reduce her abdominal discomfort and fluid retention.
Her current medication list includes:
Spironolactone 100 mg orally once daily for ascites
Furosemide 40 mg orally once daily for ascites
Propranolol 20 mg orally twice daily for portal hypertension
Lactulose 30 mL orally three times daily for hepatic encephalopathy
Rifaximin 550 mg orally twice daily for hepatic encephalopathy
Acetaminophen 500 mg orally every 6 hours as needed for pain
Ondansetron 8 mg orally twice daily for nausea
Pantoprazole 40 mg orally once daily for gastroesophageal reflux disease (GERD)
To apply the Beers criteria to Mrs. I’s medication list, we need to review each medication and compare it with the relevant indicators for her condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Spironolactone
No specific criteria
Appropriate
Aldosterone antagonists are indicated for ascites in cirrhosis
Furosemide
No specific criteria
Appropriate
Loop diuretics are indicated for ascites in cirrhosis
Propranolol
No specific criteria
Appropriate
Non-selective beta-blockers are indicated for portal hypertension in cirrhosis
Lactulose
No specific criteria
Appropriate
Osmotic laxatives are indicated for hepatic encephalopathy in cirrhosis
Rifaximin
No specific criteria
Appropriate
Antibiotics are indicated for hepatic encephalopathy in cirrhosis
Acetaminophen
Avoid in patients with liver disease or alcohol use
PIM
Acetaminophen may cause hepatotoxicity and liver failure in patients with liver disease or alcohol use
Ondansetron
No specific criteria
Appropriate
Serotonin receptor antagonists are indicated for nausea and vomiting in palliative care
Pantoprazole
Avoid in patients with life expectancy < 1 year
PIM
Proton pump inhibitors may cause hypomagnesemia, osteoporosis, infections, and rebound acid hypersecretion in patients with short life expectancy
Based on the table, we can see that Mrs. I has 2 PIMs in her medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mrs. I about her cirrhosis, ascites, portal hypertension, hepatic encephalopathy, pain, nausea, reflux, and any other concerns. Ask her about her expectations and preferences regarding her medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mrs. I, we can prioritize the medications as follows:
High priority: Acetaminophen, pantoprazole. These medications have an elevated risk of harm and low benefit for Mrs. I. They can be stopped immediately without tapering.
Medium priority: None. All other medications are appropriate for Mrs. I’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mrs. I’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mrs. I are as follows:
After stopping acetaminophen and pantoprazole, her cirrhosis, ascites, portal hypertension, hepatic encephalopathy, pain, nausea, and reflux remained well controlled and she did not experience any hepatotoxicity, liver failure, hypomagnesemia, osteoporosis, infections, or rebound acid hypersecretion. She also reported less abdominal discomfort and fluid retention.
After continuing spironolactone, furosemide, propranolol, lactulose, rifaximin, and ondansetron, her cirrhosis, ascites, portal hypertension, hepatic encephalopathy, and nausea remained well controlled. She did not experience any adverse effects from these medications.
Mrs. I was satisfied with the deprescribing process and felt more comfortable and confident with her medication regimen. She expressed gratitude to the hospice team for their care and support. She died peacefully at home a few months later.
Case Study 10: A 79-year-old man with renal failure and anemia
Meet Mr. J, a 79-year-old man who was admitted to hospice care with renal failure and anemia. He has a prognosis of less than 6 months to live, and his main goal of care is to avoid dialysis and blood transfusions.
His current medication list includes:
Erythropoietin 4000 units subcutaneously once a week for anemia
Iron sucrose 100 mg intravenously once a month for anemia
Folic acid 1 mg orally once daily for anemia
Sevelamer 800 mg orally three times daily with meals for hyperphosphatemia
Calcitriol 0.25 mcg orally once daily for secondary hyperparathyroidism
Amlodipine 5 mg orally once daily for hypertension
Metoprolol 25 mg orally twice daily for hypertension
Simvastatin 20 mg orally once daily for hyperlipidemia
Acetaminophen 500 mg orally every 6 hours as needed for pain
Morphine sulfate 10 mg orally every 4 hours as needed for pain
To apply the Beers criteria to Mr. J’s medication list, we need to review each medication and compare it with the relevant indicators for his condition and goals of care. We can use the following table to summarize our findings:
Medication
Beers Criteria
PIM or PPO
Rationale
Erythropoietin
Avoid in patients with life expectancy < 1 year
PIM
Erythropoietin may cause hypertension, thrombosis, and increased mortality in patients with short life expectancy
Iron sucrose
Avoid in patients with life expectancy < 1 year
PIM
Iron supplements may cause constipation, nausea, and drug interactions in patients with short life expectancy
Folic acid
Avoid in patients with life expectancy < 1 year
PIM
Folic acid supplements may cause masking of vitamin B12 deficiency, nausea, and drug interactions in patients with short life expectancy
Sevelamer
Avoid in patients with life expectancy < 1 year
PIM
Phosphate binders may cause constipation, nausea, and drug interactions in patients with short life expectancy
Calcitriol
Avoid in patients with life expectancy < 1 year
PIM
Vitamin D analogs may cause hypercalcemia, hyperphosphatemia, and vascular calcification in patients with short life expectancy
Amlodipine
No specific criteria
Appropriate
Calcium channel blockers are indicated for hypertension and angina
Metoprolol
No specific criteria
Appropriate
Beta-blockers are indicated for hypertension and heart failure
Simvastatin
Avoid in patients with life expectancy < 1 year
PIM
Statins may cause myopathy, hepatotoxicity, and drug interactions in patients with short life expectancy
Acetaminophen
Avoid in patients with liver disease or alcohol use
PIM
Acetaminophen may cause hepatotoxicity and liver failure in patients with liver disease or alcohol use
Morphine sulfate
No specific criteria
Appropriate
Opioids are indicated for moderate to severe pain in palliative care
Based on the table, we can see that Mr. J has 6 PIMs in his medication list. We can use the following steps to conduct the deprescribing process for these medications:
Assess the patient’s symptoms, preferences, and values. Ask Mr. J about his renal failure, anemia, hyperphosphatemia, secondary hyperparathyroidism, hypertension, hyperlipidemia, pain, and any other concerns. Ask him about his expectations and preferences regarding his medications. Explain the benefits and harms of each medication and the rationale for deprescribing.
Prioritize the medications for deprescribing. Consider the patient’s goals of care, the urgency of the problem, the potential impact of the medication change, and the feasibility of the deprescribing plan. For Mr. J, we can prioritize the medications as follows:
High priority: Erythropoietin, iron sucrose, folic acid, sevelamer, calcitriol, simvastatin. These medications have an elevated risk of harm and low benefit for Mr. J. They can be stopped immediately without tapering.
Medium priority: None. All other medications are appropriate for Mr. J’s condition and goals of care.
Low priority: None. All other medications are appropriate for Mr. J’s condition and goals of care.
Implement the deprescribing plan. Communicate the plan to the patient, the family, and the health care team. Provide clear instructions and education on how to stop or reduce the medications. Provide support and reassurance to the patient and the family. Document the plan and the reasons for deprescribing in the patient’s record.
Monitor the patient’s response. Follow up with the patient regularly to assess the effects of the medication changes. Monitor the patient’s symptoms, vital signs, laboratory tests, and quality of life. Adjust the plan as needed based on the patient’s feedback and clinical status. Address any concerns or questions from the patient, the family, or the health care team.
The outcomes of the deprescribing process for Mr. J are as follows:
After stopping erythropoietin, iron sucrose, folic acid, sevelamer, calcitriol, and simvastatin, his renal failure, anemia, hyperphosphatemia, secondary hyperparathyroidism, hypertension, hyperlipidemia, and pain remained well controlled and he did not experience any hypertension, thrombosis, increased mortality, constipation, nausea, drug interactions, masking of vitamin B12 deficiency, hypercalcemia, hyperphosphatemia, vascular calcification, myopathy, hepatotoxicity, or drug interactions. He also reported less fatigue and weakness.
After continuing amlodipine, metoprolol, acetaminophen, and morphine, his hypertension, pain, and quality of life remained well controlled. He did not experience any adverse effects from these medications.
Mr. J was satisfied with the deprescribing process and felt more comfortable and confident with his medication regimen. He expressed gratitude to the hospice team for their care and support. He died peacefully at home a few months later.
Conclusion
In this article, we have discussed how to use the Beers criteria to identify potentially inappropriate medications (PIMs) and potential prescribing omissions (PPOs) in hospice patients. We have also presented 10 case studies to illustrate the deprescribing process and the outcomes of medication changes in different scenarios.
Deprescribing is an important and challenging task in hospice care, as it requires a careful balance between the benefits and harms of each medication, the patient’s goals of care, preferences, and values, and the feasibility and acceptability of the deprescribing plan. The Beers criteria can provide a useful framework to guide the deprescribing process and to optimize the medication regimen for hospice patients.
However, the Beers criteria are not the only tool for deprescribing, and they should not be applied rigidly or blindly. They should be used in conjunction with clinical judgment, patient-centered communication, and interdisciplinary collaboration. The deprescribing process should be individualized, flexible, and responsive to the patient’s changing needs and wishes.
We hope that this article has provided some practical and helpful information for hospice clinicians and caregivers who are involved in the deprescribing process. We also hope that this article has encouraged more research and education on deprescribing in hospice care, as it is an essential component of quality palliative care.
📚 This site uses Amazon Associate links, which means I earn a small commission when you purchase books or products through these links—at no extra cost to you. These earnings help me keep this website running and free from advertisements, so I can continue providing helpful articles and resources at no charge.
💝If you don’t see anything you need today but still want to support this work, you can buy me a cup of coffee or tea. Every bit of support helps me continue writing and sharing resources for families during difficult times. 💙






 to Determine Discomfort in Your Loved One with Dementia")


