This article provides hospice nurses with practical and evidence-based strategies to discuss end-of-life care with families. The objectives of this article are to:
Discuss the benefits and barriers of end-of-life conversations for patients and families.
Provide some tips on preparing, initiating, conducting, and following up on end-of-life conversations.
Provide some examples or stories of successful end-of-life conversations using the strategies.
The Benefits of End-of-Life Conversations
End-of-life conversations are dialogues between patients, families, and healthcare providers about patients’ goals, values, and preferences regarding their end-of-life care. These conversations can improve the quality of life and care for patients and families in several ways:
Reducing stress, anxiety, and depression: End-of-life conversations can help patients and families cope with the emotional distress of facing a terminal illness and death. Patients and families can find comfort, support, and validation from each other and their healthcare providers by expressing their feelings, fears, and hopes. End-of-life conversations can also reduce the uncertainty and confusion that often accompany severe illness and enhance patients’ and families’ sense of control and autonomy.
Enhancing coping skills: End-of-life conversations can help patients and families develop and use effective coping strategies to deal with the challenges of end-of-life care. These strategies may include seeking information, making plans, setting goals, solving problems, seeking social support, using humor, and finding meaning and purpose. End-of-life conversations can also help patients and families prepare for the inevitable loss and grief that follow death and facilitate the process of acceptance and closure.
Facilitating decision-making: End-of-life conversations can help patients and families make informed and shared decisions about the medical care they want to receive or decline. By discussing their values, beliefs, and preferences, patients and families can clarify their priorities and goals of care and communicate them to their healthcare providers. End-of-life conversations can also help patients and families complete advance directives, such as living wills and health care proxies, which document their wishes and designate a surrogate decision-maker if they cannot speak for themselves.
Honoring the patient’s wishes: End-of-life conversations can help ensure their wishes are respected and honored by their healthcare providers and family members. By knowing and understanding the patient’s preferences, healthcare providers can provide care consistent with the patient’s values and goals and avoid unwanted or futile interventions. Family members can also advocate for the patient’s wishes and avoid conflicts or guilt that may arise from making decisions on behalf of the patient.
Some examples or stories of positive outcomes from end-of-life conversations are:
A 65-year-old woman with advanced lung cancer had an end-of-life conversation with her husband, daughter, and oncologist. She expressed her wish to stop chemotherapy and focus on comfort care at home. She also completed a living will and appointed her husband as her healthcare proxy. She died peacefully at home, surrounded by her loved ones, who felt relieved that they had honored her wishes and had a chance to say goodbye.
A 78-year-old man with heart failure had an end-of-life conversation with his son, daughter-in-law, and cardiologist. He expressed his wish to receive palliative care and hospice care and to avoid aggressive treatments, such as resuscitation or mechanical ventilation. He also completed a do-not-resuscitate (DNR) order and a healthcare proxy form. He enrolled in a hospice program and received pain and symptom management, as well as emotional and spiritual support. He died comfortably in a hospice facility, with his son by his side, who felt grateful that his father had a good death.
A 54-year-old woman with ALS had an end-of-life conversation with her husband, two sons, and a neurologist. She expressed her wish to receive life-prolonging treatments, such as a feeding tube and a ventilator, as long as they improved her quality of life. She also completed a living will and a health care proxy form. She received home care and assistive devices that helped her communicate and function. She died at home, with her family and friends around her, who felt proud that she had lived her life to the fullest.
The Barriers to End-of-Life Conversations
End-of-life conversations are often complex and sensitive for hospice nurses, patients, and families. Many barriers prevent hospice nurses from initiating or conducting end-of-life conversations with families, such as:
Lack of time and opportunity: Hospice nurses may have limited time and opportunity to engage in end-of-life conversations with families due to heavy workloads, competing demands, and frequent interruptions. They may also face challenges finding suitable settings, timing, and privacy for these conversations.
Lack of skills and confidence: Hospice nurses may lack the skills and confidence to communicate effectively with families about end-of-life issues. They may feel uncomfortable, unprepared, or inexperienced in initiating, conducting, and following up on these conversations. They may also have difficulty dealing with families’ emotional reactions, such as anger, denial, or guilt.
Lack of support and resources: Hospice nurses may lack the support to facilitate end-of-life conversations with families. They may not have access to adequate training, education, or mentoring on end-of-life communication. They may also not have access to interdisciplinary teams, palliative care specialists, or other professionals who can assist them in these conversations.
Lack of awareness and understanding: Hospice nurses may lack awareness and understanding of the importance and benefits of end-of-life conversations for patients and families. They may not recognize the cues or triggers that indicate the need for these conversations. They may also not understand patients’ and families’ values, preferences, goals, or the cultural, religious, or ethical factors influencing their end-of-life decisions.
Lack of agreement and collaboration: Hospice nurses may lack agreement and cooperation with other healthcare providers, patients, and families regarding end-of-life conversations. They may face conflicts or disagreements with other healthcare providers about the prognosis, treatment options, or goals of care. They may also face resistance or reluctance from patients or families who do not want to talk about end-of-life issues or who have different expectations or wishes.
These barriers can have negative impacts on the patient’s and family’s well-being and satisfaction with care, such as:
Reduced quality of life and care: Patients and families may not receive care consistent with their values and goals without end-of-life conversations. They may receive unwanted or futile interventions that cause more harm than benefit. They may also suffer from unrelieved pain and symptoms, emotional distress, and spiritual distress.
Reduced decision-making and autonomy: Without end-of-life conversations, patients and families may be unable to make informed and shared decisions about the medical care they want to receive or decline. They may not complete advance directives, such as living wills or health care proxies, which document their wishes and designate a surrogate decision-maker. They may also lose a sense of control and autonomy over their end-of-life care.
Reduced coping and bereavement: Without end-of-life conversations, patients and families may not have the opportunity to cope with the emotional, psychological, social, and spiritual challenges of facing a terminal illness and death. They may not have the chance to express their feelings, fears, and hopes or to find comfort, support, and validation from each other and their healthcare providers. They may also have difficulty in preparing for the inevitable loss and grief that follows death and may experience prolonged or complicated bereavement.
Some examples or stories of negative outcomes from the lack of end-of-life conversations are:
A 70-year-old man with advanced prostate cancer was admitted to a hospice facility after a series of hospitalizations and complications. He had never had an end-of-life conversation with his wife, son, or hospice nurse. He was in severe pain and distress, but he did not want to take any medications or treatments that would make him sleepy or unconscious. He also did not want to talk about his condition or his wishes. His wife and son were confused about what to do for him. They did not know if he wanted to be resuscitated or intubated if his condition worsened. They also did not know if he wanted to have a funeral or a cremation. They felt helpless, guilty, and angry/
A 60-year-old woman with end-stage heart failure was transferred to a hospice facility after a cardiac arrest and a prolonged stay in the intensive care unit. She had never had an end-of-life conversation with her husband, daughter, or hospice nurse. She was unconscious and dependent on a ventilator and a feeding tube. Her husband and daughter had different opinions about her care. Her husband wanted to continue the life-sustaining treatments, hoping for a miracle. Her daughter wanted to withdraw from the treatments, respecting her mother’s dignity. They argued and blamed each other for their mother’s situation. They also felt betrayed and abandoned by the healthcare providers who had not discussed the prognosis or the options with them.
A 50-year-old woman with ALS had an end-of-life conversation with her husband but not with her two teenage sons or her hospice nurse. She expressed her wish to die at home with the help of physician-assisted dying. She also completed a living will and a health care proxy form. However, she did not tell her sons about her decision or condition. She wanted to protect them from the pain and the reality of her illness. Her sons were unaware of her situation and her wishes. They were shocked and devastated when they learned that their mother had died at home with a lethal injection. They felt angry, guilty, and depressed.
The Strategies for End-of-Life Conversations
End-of-life conversations are essential for hospice nurses to provide patient-centered and family-oriented care. However, these conversations can be challenging and complex, requiring specific skills and strategies. Here are some practical and evidence-based strategies that hospice nurses can use to overcome the barriers and engage in effective end-of-life conversations with families:
Prepare for the conversation: Hospice nurses should prepare themselves by reviewing the patient’s medical history, prognosis, and treatment options. They should also assess the patient’s and family’s readiness, willingness, and preferences for end-of-life discussions. They should identify the goals and objectives of the conversation and plan the key messages and questions they want to convey and ask. They should also seek support and guidance from their colleagues, mentors, or palliative care specialists if needed.
Initiate the conversation: Hospice nurses should initiate the conversation by finding a suitable setting, timing, and privacy for the discussion. They should also invite the patient and family members who need to be involved and obtain their consent for the conversation. They should introduce themselves and their role and explain the purpose and importance of the conversation. They should also establish rapport and trust with the patient and family using empathy, active listening, and open-ended questions.
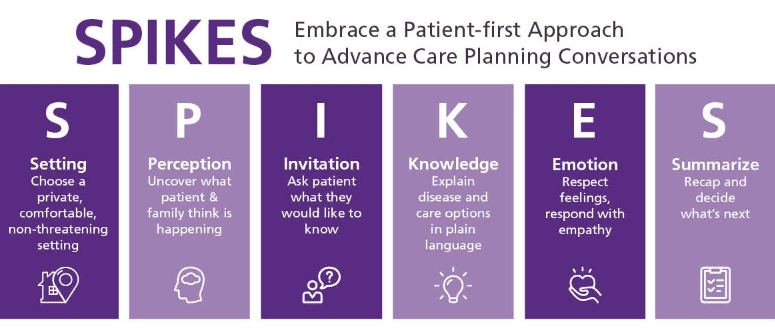
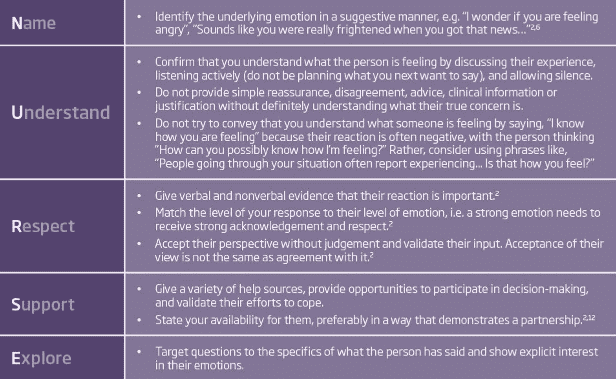
Conduct the conversation: Hospice nurses should follow a structured and flexible approach, such as the SPIKES protocol or the NURSE mnemonic. They should explore the patient’s and family’s understanding, expectations, and concerns about the illness and end-of-life care. They should provide information and education that is accurate, honest, and tailored to the patient’s and family’s needs and preferences. They should elicit and respect the patient’s and family’s values, beliefs, and goals of care and help them make informed and shared decisions. They should also address the patient’s and family’s emotional and spiritual needs and offer support and resources.
Follow-up on the conversation: Hospice nurses should follow up by documenting and communicating the outcomes and decisions of the discussion to the patient, family, and other healthcare providers. They should also monitor and evaluate the patient’s and family’s satisfaction and understanding of the conversation and the care plan. They should also provide ongoing and regular communication and feedback to the patient and family and revisit and revise the conversation and the care plan as needed.
Some examples or stories of successful end-of-life conversations using the strategies are:
A hospice nurse prepared for an end-of-life conversation with a 75-year-old woman with advanced ovarian cancer and her daughter. She reviewed the patient’s medical records and learned that she had declined further chemotherapy and opted for comfort care. She also assessed the patient’s and daughter’s readiness for the conversation and found they were open and willing to talk. She planned to discuss the patient’s goals and preferences for end-of-life care and to complete an advance directive with her.
The hospice nurse initiated the conversation by finding a quiet and comfortable room in the hospice facility where the patient was staying. She invited the patient and her daughter to join her and asked for their permission to discuss end-of-life issues. She introduced herself and explained that she wanted to help them plan the best possible care for the patient. She also expressed empathy and compassion for their situation and asked them how they felt.
The hospice nurse conducted the conversation by using the SPIKES protocol. She first assessed the patient’s and daughter’s perception of the patient’s condition and prognosis. She then obtained their invitation to share the information they wanted to know. She then gave them the information clearly and sensitively, using simple and non-technical language. She then addressed their emotions and reactions, using the NURSE mnemonic to name, understand, respect, support, and explore their feelings. She then explored their values and goals of care, asking them what mattered most to them and what they hoped for and feared. She then helped them make decisions that aligned with their values and goals, such as choosing a do-not-resuscitate (DNR) order and a healthcare proxy. She also provided them with education and resources on end-of-life care and hospice services.
The hospice nurse followed up on the conversation by documenting and communicating the patient’s and daughter’s wishes and decisions to the hospice team and the patient’s primary care physician. She also checked in with them regularly and asked them if they had any questions or concerns. She revisited and revised the conversation and the care plan as the patient’s condition changed and new issues arose.
The patient and her daughter were satisfied and grateful for the hospice nurse’s end-of-life conversation. They felt that they better understood and controlled the patient’s care and that their wishes were respected and honored. They also felt more prepared and supported for the patient’s death.
Conclusion
This emphasizes the importance of end-of-life conversations for hospice nurses to provide patient-centered and family-oriented care. It discusses the benefits, barriers, and strategies for effective end-of-life conversations. The benefits of such discussions include reducing stress, enhancing coping skills, facilitating decision-making, and honoring the patient’s wishes. On the other hand, barriers such as lack of time, talent, support, awareness, and collaboration can lead to adverse outcomes, impacting the patient’s and family’s well-being and satisfaction with care.
The article provides practical and evidence-based strategies for hospice nurses to overcome these barriers, including preparing for the conversation, initiating it, conducting it, and following up on it. It also includes examples of successful end-of-life conversations using these strategies, highlighting the positive impact of effective communication on patients and families.
In conclusion, the article underscores the significance of end-of-life conversations in providing compassionate and person-centered care. Addressing the challenges and offering practical strategies, it aims to empower hospice nurses to engage in effective end-of-life conversations, ultimately enhancing the quality of care for terminally ill patients and their families.
All the Blues in the Sky by Renée Watson – About a 13-year-old whose best friend dies on her birthday, exploring grief through counseling group experiences.
The Truth as Told by Mason Buttle by Leslie Connor – Chronicles a boy dealing with a friend’s death, a learning disability, and community judgment.
The Year of the Rat by Clare Furniss – A 15-year-old coping with her mother’s death during childbirth and caring for her baby sister.
The Dougy Center offers extensive free resources, including activity sheets, tip sheets, and guidance for children and families. They provide age-appropriate materials and have partnered with Sesame Street on grief resources.
Winston’s Wish provides comprehensive bereavement support for children up to age 25, including online chat, phone support, and downloadable resources. It also offers specialized guidance for different types of loss.
Sesame Street Communities: Helping Kids Grieve features interactive videos with Elmo and other characters, activities for expressing feelings, and family guidance. All resources are free and available in multiple languages.
The National Alliance for Children’s Grief (NACG) provides educational toolkits, connects families to local support services, and offers professional development for those working with grieving children.
GriefShare helps locate local grief support groups for families and provides daily email encouragement for those processing loss.
Enhanced Online Resources for Teens
Specialized Teen Platforms
Talk Grief—Winston’s Wish operates this dedicated online space for teenagers and young adults aged 13-25. It features peer stories and professional support.
Teenage Grief Sucks – A teen-run website opening conversations about grief where teens can read candid stories and share their own experiences.
Actively Moving Forward – A national network specifically created for grieving young adults, addressing the unique challenges of this age group.
The Dinner Party – Young adults in nearly 100 cities worldwide meet for dinner, creating community for emerging adults who’ve experienced loss.
Comprehensive Teen Support Centers
The Dougy Center Teen Resources provides age-specific materials, including tip sheets, that acknowledge “grief usually does what it wants” and doesn’t follow rules or schedules. They emphasize that there’s no right or wrong way to grieve.
Hospice of the Valley Teen Resources offers specialized materials addressing how teens grieve differently than adults, sudden versus expected death, and losing siblings or friends.
Children’s Room Teen Program provides peer support groups and activities specifically for teens to connect around shared interests while processing grief.
Interactive Support Options
Winston’s Wish offers immediate support through live chat, helpline, and text services – no waiting lists required. They also provide one-to-one sessions with bereavement specialists for teens 13 and older.
HEART Play for Young Adults connects late high school and college-aged individuals, providing space to discuss challenges of graduation, leaving home after loss, and meeting new people.
Educational Resources for Teens and Families
The JED Foundation provides mental health resources showing teens how they can support one another and overcome challenges during the transition to adulthood.
Eluna Network offers grief resources organized by specific age ranges, including detailed developmental information and support strategies for both middle school and high school students.
National Alliance for Children’s Grief provides educational toolkits and connects families to local services, with materials specifically designed for adolescent grief.