Empowering Hospice Nurses: Conquering Medicare Audits and Improving Documentation for Better Patient Care
Published on July 29, 2023
Updated on June 16, 2024
Published on July 29, 2023
Updated on June 16, 2024
Table of Contents
The Centers for Medicare and Medicaid Services (CMS) created the program Targeted Probe and Educate (TPE) to perform audits in November 2017 to improve the review and education process, reduce appeals, decrease provider burden, and reduce and prevent improper payments. Medical reviews for hospice organizations went to full speed in late 2021.
On Wednesday, July 12, 2023, a compliance team from our corporate office met with all our nurses covering several counties in South Central Pennsylvania to demonstrate why tens of thousands of dollars of hospice services were being denied. They reminded us of the bureaucracy of Medicare, where third-party auditors without a proper (by our standards) healthcare background were making the decisions to approve or deny bills based on their layperson reading of the documentation we as nurses provide them by what is in our visit narratives.
These auditors read what we write, and the ONLY context they get is what we write. They are purposefully looking to deny! They are purposefully looking to reject based on what YOU and I write about our patients. All it takes is just one visit note that gives the impression the person has longer than six months to live!… and then the entire claim is subject to denial. This is typically in multiples of $10,000! This hurts the patient and family! This hurts our agency! This hurts our reputation as hospice nurses!
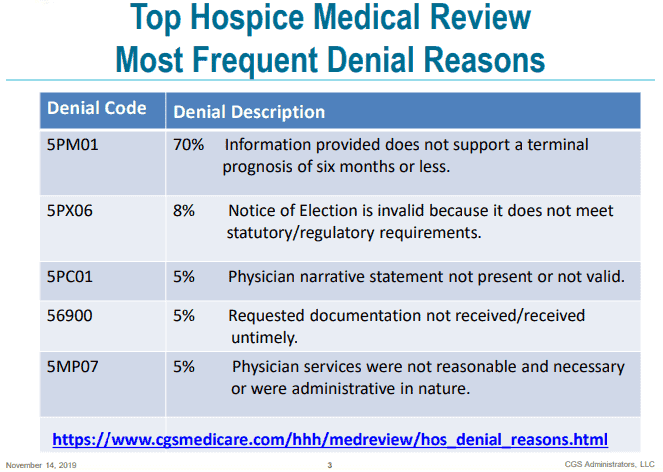
The number one reason for claim denials for Hospice continues to be documentation not supporting the six-month or less terminal prognosis.
In the last few years, I came across Shelley Henry, RN, CPHRM, CHPN—President—The Amity Group, on Facebook, where she posts tips for hospice nurses several times per week. It is from Shelley that I learned to start documenting “disoriented x3” vs. “oriented x1” and the value of negative-based presentations, as being terminally ill involves negative (downward) changes of condition.
This led me to obtain two of Shelley’s developed products, “A Hospice Nurse’s Guide to Hospice Documentation” and “A Supplemental Guide to Hospice Documentation,” as part of the Hospice Documentation Master Bundle. I shared a review of this bundle on July 17, 2023.
Since that review, I’ve been working on improving my documentation with the personal goal that none of my eligible patients would have their claims denied because my documentation did not support a picture of six months or less terminal diagnosis.
While keeping in mind today is July 29, 2023, with less than 30 days of practice, please allow me to share some before and after registered nurse visit narratives whose only modification for public posting is to ensure the patient’s and family’s privacy. Also, the narratives will be all upper case (I’m not screaming or yelling) as that’s how the software stores the narratives. Finally, not every terminal disease is included in the documentation bundle; however, the examples provided are so thorough that they are easy to adapt to the terminal disease process not included in the bundle for which you may have cases to manage.
VISIT NARRATIVE:
__-YEAR-OLD WHITE MALE ON SERVICE FOR ALZHEIMER’S
CG _______ REPORTS PT INCREASED SLEEPING. WIFE DEB REPORTING SYMPTOMS WELL MANAGED.
PT SLEEPING UPON ARRIVAL AND SLEPT THROUGH ASSESSMENT AND VISIT. SALLOW/ILL COMPLEXION, GLOSSY/MOIST SKIN, VISIBLE BONY PROMINENCES, CRUNCHED UP IN BED R/T CONTRACTURES, LIMITED RANGE OF MOTION, AND STIFFNESS.
AFEBRILE 97.3. LUNGS CTA, RR 20, SPAO2 92%, RASPY BREATHING. MURMUR, 64 RADIAL. BP 130/78 RIGHT WRIST LAYING. NO EDEMA. INCONTINENT OF BLADDER AND BOWEL. UNABLE TO AMBULATE BEING BEDBOUND REQUIRING COMPLETE CARE.
CONTRACTURES: BILALERAL UPPER ARM CONTRACTURES AT THE ELBOW. BILATERAL CONTRACTURES AT KNEE ~10 TO 15 DEGREES. CONTRACTURES ON BOTH HANDS WHERE FINGERS ARE HARDER TO SEPARATE AND MOVE.
BILATERAL FOOT DROP: ~10 DEGREE ANGLE.
NO REFILS NEEDED.
EDUCATION PROVIDED ON DISEASE PROCESS AND PROGRESSION.
VISIT NARRATIVE:
__-YEAR-OLD WHITE MALE ON SERVICE FOR ALZHEIMER’S
CG _______ REPORTS ON/OFF PERIODS OF AGITATION/COMBATIVE BEHAVIORS TO GIDDY TO IN BETWEEN; “EACH HOUR IS DIFFERENT.”
PT SLEEPING IN A CRUNCHED-UP POSITION IN BED UPON ARRIVAL. SKIN MOIST, VISIBLE BONY PROMINCES.
DUE TO THE PROGRESSION OF TERMINAL ALZHEIMERS, PT HAS BILATERAL UPPER AND LOWER CONTRACTURES ALONG WITH FOOT DROP, LIMITED RANGE OF MOTION BILATERALLY UPPER AND LOWER INCLUDING BACK AND NECK. WHEN PT IS AWAKE, DISORIENTED X3 ONLY ABLE TO RECOGNIZE HIS NAME WHEN HIS NAME IS REPEATED MULTIPLE TIMES; UNABLE TO SPEAK ANY INTELLIGIBLE WORD RELATED TO THE SITUATION. WHEN HE TRIES TO SPEAK, THE WORDS ARE EITHER MUBLED INCOHRENT OR NONSENCIAL WITH LAUGHTER OR RAGE. PT HAVING INCREASED HALLUCINATIONS OF ANIMALS AND PEOPLE. PT RARELY OPENS HIS EYES COMPLETELY.
PT UNABLE TO EXPRESS HIS NEEDS, DESIRES, OR PAIN; PAINAD 0/10. HOSPICE PLAN OF CARE INVOLVES USING 0.5 MG LORAZEPAM IF THE NONPHARMALOGICAL METHODS FAIL; AND FAMILY LEANS TOWARDS THE NONPHARM METHODS THAT HAVE BEEN EFFECTIVE LESS TWO OCCASSIONS WHERE THEY DID USE THE LORAZEPAM.
INCONTINENT OF BLADDER AND BOWEL. UNABLE TO AMBULATE BEING BEDBOUND REQUIRING COMPLETE CARE INCLUDING FEEDING. LACK OF TRUNK CONTROL AS THE PATIENT LEANS TO HIS LEFT. FUNCTIONAL ASSESSMENT 30/30.
PT DID NOT WAKE THROUGH ENTIRE VISIT.
NO REFILS NEEDED.
EDUCATION PROVIDED ON DISEASE PROCESS AND PROGRESSION. HOSPICE PLAN OF CARE REVIEWED AND ACCEPTED BY WIFE
VISIT NARRATIVE
__-YEAR-OLD WHITE MALE ON SERVICE FOR COPD
FRIEND AND CG _______ PRESENT FOR THE VISIT.
SINCE LAST WEDNESDAY, 6/28 THE PATIENT USED ~10 ML (200 MG) LIQUID MORPHINE (~26 ML TO ~16 ML). PT REPORTED ABDOMINAL DISCOMFORT WITH LOSE STOOLS MONDAY, 7/3 INTO TUESDAY, 7/4. ONE SLICE TOAST MONDAY AND NOTHING ELSE R/T ABDOMINAL DISCOMFORT W/O NV. PT REPORTED FEELING BETTER BY TUESDAY AFTERNOON.
PT STARTED 15 MG MS CONTIN ER FRIDAY, 6/30 EVENING WITH PT REPORTING HE USED THE LIQUID MORPHINE BETWEEN 6/28 AND FRIDAY EVENING AND ONCE SINCE THEN FOR BREAKTHROUGH.
PT IS THIN WITHOUT BEING CACHEXIC. CHRONIC SKIN INJURY UNDER HIS RIGHT EYE. AFEBRILE 97.3. DISORIENTED X2 WITH FORGETFULNESS. LUNGS WHEEZY, RR 20, SPAO2 97% ON 3L. MUFFLED HEART SOUNDS, PULSEOX 86. MANUAL BP LEFT ARM SITTING 138/70. NO EDEMA. CONTINENT OF BLADDER AND BOWEL. AMBULATES WITH O2.
NO REFILLS NEEDED.
EDUCATION PROVIDED ON DISEASE PROCESS AND PROGRESSION.
VISIT NARRATIVE
_______ IS A __-YEAR OLD WHITE MALE WITH A TERMINAL HOSPICE DIAGNOSIS OF COPD AND THE SECONDARY COMPLICATIONS OF SHORTNESS OF BREATH, FATIGUE, DIFFICULTY IN WALKING. COMORBID CONDITIONS THAT FURTHER CONTRIBUTE TO DECLINE INCLUDE THE PERSONAL HISTORY OF MALIGNANT NEOPLASM OF BRONCHUS AND LUNG. PT REPORTS HE WAS HOSPITALIZED PRIOR TO HOSPICE WITH CONGESTIVE HEART FAILURE AND THAT’S WHY HE IS ON THE FUROSIDIDE PRN. PT LIVES WITH TWO FRIENDS, _______ AND _______.
UPON ARRIVAL, DOOR OPEN FOR THE WRITER AS DUE TO THE PROGRESSION OF TERMINAL COPD LIVES MOSTLY A CHAIR AND BED EXISTENCE FREQUENTLY OUT OF BREATH IF HE WERE TO ANSWER THE DOOR APPROXIMATELY ~15 FEET AWAY FROM THE RECLINER HE NORMALLY SITS. PT REPORTS THAT WHEN HE TRIES TO HELP WITH CHORES AROUND THE HOME, HE HAS TO TAKE 10 MINUTE BREAKS FREQUENTLY IN ORDER TO CATCH HIS BREATH.
DUE TO THE PROGRESSION OF TERMINAL COPD, THE PT HAS WEAK INSPIRATORY EFFORT WITH MINIMAL LUNG EXPANSION USING ACCESORY MUSCLES WITH EACH BREATH; LUNG SOUNDS ARE DIMINISHED BILATERALLY WITH POOR AIR EXCHANGE PT USING DUONEBS FOUR TO FIVE TIMES PER DAY WHICH IS AN INCREASE OF ONE ADDITIONAL TIME COMPARED TO LAST RECERTIFICATION. ~20 MINUTES OFF OXYGEN, THE PATIENT’S SATURATION CAME DOWN TO 69% ON ROOM AIR.
WHILE PT DID GAIN 0.5 POUNDS THIS CERT PERIOD, HE REPORTS THAT AFTER HIS FALL ON 7/15 HE WAS BARELY EATING AND THEN THIS PAST WEEK FELT BETTER AND OVERATE.
PT IS 5′ 9″ TALL, THIN ALMOST CACHEXIC IN APPERANCE, BARREL CHEST, CONCAVE ABOMDINAL AREA WITH A CHRONIC, NON-HEALING SKIN ULCERATION UNDER HIS RIGHT EYE. THE SKIN TEAR ON HIS LEFT ELBOW FROM THE FALL IS NOW SCABBED OVER. PT HAS VISIBLE BONY PROMINENCES AND HAS LOST 2 CM (8.33%) OF RMAC SINCE THE LAST CERTIFICATION.
PT UNABLE TO AMBULATE WITHOUT O2 WITH DECREASED MUSCLE COORDINATION, TROUBLE AROUND TURNS WITH A MORE UNSTEADY GATE.
TC TO _______AT _______ PHARMACY TO ASK FOR TWO BOXES OF DUONEBS FOR AM DELIVERY TOMORROW. TC TO CG _______ TO UPDATE.
HOSPICE PLAN OF CARE REVIEWED WITH PATIENT AND CG _______ WITH NO REVISION NECESSARY FOR THIS VISIT.
VISIT NARRATIVE:
__-YEAR-OLD BLACK FEMALE ON SERVICE FOR END-STAGE PARKINSONS
NURSE _______ DENIES PT CHANGE OF CONDITION OR MED CHANGES SINCE LAST VISIT.
SISTER _______ SHOWED UP SHORTLY AFTER THE WRITER STARTED THE VISIT, REPORTING THE PT IS TOLERATING BEING FED AND IS NOW RECEIVING SLIGHTLY LARGER PORTION SIZES AND TOLERATING THE AMOUNT.
PT IS LYING IN BED, WAKES TO LIGHT STIMULI, DENIES PAIN, AND APPEARS COMFORTABLE IN NO APPARENT DISTRESS; PAINAD 0/10. COMPLEXION APPROPRIATE FOR AGE AND RACE. THEIR LOWER LIP IS EXTENDED, AND PT HAS POOR MOUTH CONTROL; SHE NEEDS ASSISTANCE IN EATING WITH SOMEONE HOLDING HER LOWER CHIN TOWARDS HER UPPER TO CLOSE HER MOUTH AND HELP HER CHEW.
AFEBRILE 97.9. DISORIENTED X3. LUNGS CTA, RR 20, SPAO2 77% ON ROOM AIR; COOL HANDS. WEAK HEART SOUNDS AT 30X AMPLIFICATION. RADIAL 77. BP 107/77 RIGHT WRIST LAYING. NO EDEMA. INCONTINENT OF BLADDER AND BOWEL. UNABLE TO AMBULATE, BEING BEDBOUND, REQUIRING COMPLETE CARE.
BILATERAL KNEE CONTRACTURES AT ~45 DEGREES.
EDUCATION PROVIDED ON DISEASE PROCESS AND PROGRESSION.
__-YEAR-OLD BLACK FEMALE ON SERVICE FOR END-STAGE PARKINSONS
NURSE _______ REPORTED DC OF VIT D2 AND TRAMADOL. HOSPICE MAR RECONCILED.
PT IN BED UPON ARRIVAL SLEEPING WAKES TO LIGHT STIMULI. LOWER LIPS ARE PUFFY AND EXTENDED SUCH THAT THE PT REQUIRES HER LOWER JAW TO BE HELD SHUT TO HELP HER TO CHEW AND BE FED. BILATERAL LOWER CONTRACTURES AT THE KNEE AT APPROXIMATE 50-DEGREE ANGLES INCREASED FROM 45 DEGREES THE PREVIOUS VISIT.
DUE TO THE PROGRESSION OF TERMINAL END-STAGE PARKINSONS, PTS HAVE VARIOUS DEGREES OF STIFFNESS AND A LIMITED RANGE OF MOTION IN THE UPPER AND LOWER BILATERAL EXTREMITIES. THE ELBOW TO THE HANDS IS SLIGHTLY FLACCID, THE ELBOW TO THE SHOULDERS IS TIGHT AND STIFF, AND THE LOWER EXTREMITIES ARE STIFF.
NEUROLOGICALLY PT IS DISORIENTED X3 WITH FORGETFULNESS. PT UNABLE TO PROPERLY EXPRESS PAIN; PAID 0/10.
CARDIOPULMONARY: PT HAS WEAK HEART SOUNDS AT 30X AMPLIFICATION; HRR. UTA BP X2 ATTEMPS.
PT IS INCONTINENT OF BLADDER AND BOWEL.
DUE TO THE PROGRESSION OF TERMINAL ILLNESS, PT IS A COMPLETE FEED AND COMPLETE CARE BEING BEDBOUND, UNABLE TO AMBULATE WITHOUT A HOYER LIFT TO TRANSFER. FUNCTIONAL ASSESSMENT 27/30.
TC TO POA _______ TO UPDATE; HIPAA-APPROPRIATE VM LEFT
UNIT MANAGER _______ UPDATED.
VISIT NARRATIVE:
__-YEAR-OLD WHITE FEMALE ON SERVICE FOR SDB
DON _______ DENIES PT CHANGE OF CONDITION SINCE THE LAST VISIT.
PT IN BRODA ELITE WAS AWAKE AND ALERT UPON ARRIVAL WITH FACILITY HHA _______, REPORTING PT WAS FED BREAKFAST AND ATE HER BREAKFAST, INCLUDING LIQUIDS.
PT HAS FACIAL THINNING, WEARS GLASSES, IS HARD OF HEARING, AND DOES NOT USE HEARING DEVICES. WORD SALAD INVOLVING HALLUCINATORY EVENTS OR OTHERWISE UNREALTED TO ANY QUESTIONS, SITUATION, ETC. PT FELL ASLEEP ~15 MINUTES INTO THE VISIT ONCE THE PHYSICAL ASSESSMENT WAS COMPLETED.
LEFT EYELIDS, UPPER AND LOWER, ARE BACK TO BASELINE COMPARED TO FRIDY’S VISIT.
AFEBRILE 97.4. DISORIENTED X3 WITH FORGETFULNESS, HALLUCINATIONS/DISORIENTATION. LUNGS CTA, RR 18 SPAO2 95% ON ROOM AIR; INTERMITTENT COUGH. HRR, RADIAL 85. BP 127/81 RIGHT WRIST SITTING. NO EDEMA. INCONTINENT OF BLADDER AND BOWEL. UNABLE TO AMBULATE, REQUIRING A HEAVY TWO-ASSIST OR HOYER LIFT TO TRANSFER. WC/CHAIR/BEDBOUND REQUIRING COMPLETE CARE INCLUDING FEEDING.
TC TO DGT _______ TO UPDATE.
__-YEAR-OLD WHITE FEMALE ON SERVICE FOR SDB
DON _______ UPDATED THE HOSPICE POC, INCLUDING A REMINDER FOR MONTHLY WEIGHTS. _______ UPDATED THE SYSTEM TO ASK THE CGs TO GET A WEIGHT IN THE NEAR FUTURE.
OUR CNA _______ REPORTED THAT WHILE SHE WAS FEEDING THE PT, PT FREQUENTLY HALLUCINATED.
PT SITTING IN BRODA CHAIR UPON ARRIVAL. PT DOES NOT APPEAR AWARE OF THE ARRIVAL AND OFFERS NO INTERACTION WITH THE ENVIRONMENT. THE WRITER SAID HELLO AND ASKED HOW THE PATIENT IS DOING. DUE TO THE PROGRESSION OF THE END-STAGE TERMINAL SENILE DEGENERATION OF THE BRAIN, THE PATIENT IS DISORIENTED TO PLACE, TIME, AND EVENTS. SPEECH IS NONSENSICAL, WITH NO RELATIONSHIP TO THE QUESTIONS ASKED OR THE CIRCUMSTANCES. PT IS UNABLE TO EXPRESS THOUGHTS, FEELINGS, OR NEEDS EFFECTIVELY. THE HOSPICE INTERVENTIONS OF 650 MG TYLENOL BID AND 25 MG TRAMADOL HS ARE EFFECTIVELY MANAGING THE PATIENT’S PAIN. PAINAD 0/10.
DUE TO THE PROGRESSION OF THE END-STAGE TERMINAL SENILE DEGENERATION OF THE BRAIN, THE PATIENT IS CHAIR/BEDBOUND AND IS NON-WEIGHT BEARING, REQUIRING MAXIMUM ASSISTANCE TO TRANSFER. WHILE IN HER CHAIR, PT HAD MINIMAL INTERACTION WITH THE ENVIRONMENT AND FELL ASLEEP SHORTLY AFTER THE WRITER ARRIVED. PT HAS NO NECK CONTROL AND PT’S HEAD TOWARDS CHEST. PT REQUIRES A BRODA CHAIR TO REDUCE THE RISK OF FALLS.
SKIN IS COOL TO TOUCH, DRY, THIN, AND FRAGILE. PROTECTIVE POSITIONING REQUIRED TO REDUCE SKIN BREAKDOWN RISK AND PROTECT THE PATIENT’S JOINTS AS BONY PROMINENCES ARE VISIBLE.
PT REQUIRES COMPLETE CARE, INCLUDING FEEDING A MECHICAL SOFT, THIN LIQUID DIET. PT IS SHOWING SIGNS OF REDUCED APPETITE, NO LONGER COMPLETING 100% OF THREE ADULT-SIZED MEALS BUT NOW AVERAGING 50% TO 75% OF THOSE THREE MEALS. PT REQUIRES FREQUENT ENCOURAGEMENT AND QUING TO EAT. PT IS INCONTINENT OF BLADDER AND BOWEL. FUNCTIONAL SCALE 27/30.
THE CURRENT HOSPICE PLAN WAS REVIEWED WITH DIRECTOR _______, WHO IS IN AGREEMENT WITH THE PLAN; NO REVISIONS ARE TO BE MADE AT THIS TIME.
TC TO DGT ______ TO UPDATE; HIPAA-APPROPRIATE VM LEFT
Don’t let bureaucratic hurdles stand in the way of providing the best hospice care for your patients! The recent surge in audits and claim denials has put immense pressure on hospice nurses like us, but there’s a way to turn the tide in our favor.
“A Hospice Nurse’s Guide to Hospice Documentation” and “A Supplemental Guide to Hospice Documentation” – are essential tools developed by Shelley Henry, a seasoned expert in the field. These guides are part of the comprehensive Hospice Documentation Master Bundle that can revolutionize how you document patient care.
Imagine the satisfaction of knowing that your documentation is foolproof and supports the critical six-month or less terminal prognosis. Following Shelley’s expert advice, you can effectively communicate your patient’s needs to third-party auditors and avoid those devastating claim denials that hurt both patients and your agency.
With less than 30 days of practice, you can immediately begin implementing these invaluable techniques. Don’t miss this opportunity to enhance your documentation skills and safeguard the care you provide to those in need.
Let’s rise above the challenges and embrace a future where our documentation is unparalleled, ensuring the best outcomes for our patients and the hospice community. Take the next step toward excellence – get the Hospice Documentation Master Bundle and experience the difference firsthand! Your patients and your agency will thank you.
The author is not related to Shelley Henry or any family member, is not employed or otherwise contracted by the Amity Group, and will not receive any financial benefit from anyone purchasing these products. None of the links on this page are affiliate links.
Hospice Top Medical Review Denial Reason Codes
Review of the Hospice Documentation Master Bundle
Hospice Nurses Speak: How to Attract Us, Keep Us, or Lose Us
The Amity Group Documentation Videos – wonderful tips – on Tic Tok
The Amity Group featured on CW39 Houston








