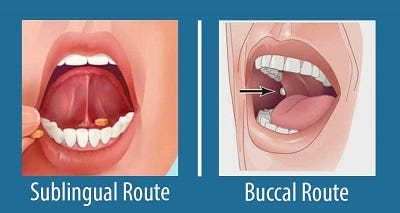
Buccal vs Sublingual for Liquid Medications
Published on April 18, 2021
Updated on May 23, 2024
Published on April 18, 2021
Updated on May 23, 2024
Your dying patient has lost their gag reflex as part of the dying process. One of the questions I implore you to ask yourself is, what’s the safest route to administer liquid medications? Before even answering this question, unless contraindicated, ensure the patient’s head of the bed is at least at a 30 to 45-degree angle (I prefer the latter).
The buccal route is the safest route to administer liquid medications at the end of life, in my experience. In practice, I strongly encourage you, as well as the families we mutually teach, to give any liquid medications on the side of the mouth least likely to have spillage — this depends on the position of the patient — and slowly, over time, giving the medication in 0.25 ml increments allowing for the absorption of the medication switching cheeks as applicable.
As you teach families to administer liquid morphine, haloperidol, melted, or liquid lorazepam, encourage them to take their time rather than speedily pushing the plunger of the syringe. As I teach families and am now teaching you, I also remind them of the uncomfortable feeling of a thermometer in their mouth (if kept there too long) to encourage them to remove the syringe here and there and then re-enter the buccal space as they are taking their time to give whatever is the full dose.
Now, very recently, on Friday, April 16, 2021, I was in a hot mess of a situation where I was caring for a dying patient who came home from the hospital with only liquid oxycodone 5 mg per 5 ml even though several hours earlier, I confirmed with the RN hospital nurse on duty they would be sending Roxanol—Haloperidol and lorazepam at home with the patient. I had to be a form of MacGyver, using what I had on hand to help the extremely restless, agitated patient just using 5 ml of liquid oxycodone at a time. To emphasize the importance of going slow with liquid medications when the patient is dying, giving 5 ml took close to ten minutes, including pauses, as the syringe I was using was a 5 ml syringe whose barrel was greater in diameter than the 1 ml syringe and with the agitated and restless patient needed to be removed often.
From Ellen Seniuk, a good reminder: When doing this, keep the head of the bed up and use both sides of the mouth. Keep the head of the bed elevated for several minutes after administering.
Has your experience been the same regarding buccal being better than sublingual? And if this is new for you, have you tried the suggestions above? How have they worked for you?
Sublingual and Buccal Medication Administration
Various articles with tips for nurses






